


All Global Research articles can be read in 51 languages by activating the Translate Website button below the author’s name.
To receive Global Research’s Daily Newsletter (selected articles), click here.
Click the share button above to email/forward this article to your friends and colleagues. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
***
What do we do when our agencies, institutions, and the very machinery of democratic government have been commandeered by profit interests and weaponized against the people? We call for a new Nuremberg.
Over the last three years, the FDA, the CDC, the NIH, the NIAID, the AMA and U.S. Public Health Service, and a group of over 3900 American local and legacy media partners[1 2 3] engaged in a conspiracy of misinformation and misdirection which led to the preventable[4] deaths of almost 3.4 million people globally, and the preventable injuries and hospitalizations of millions or billions more. It opened the gate for the administration of over 13.5 billion doses of the world’s deadliest product ever marketed as a vaccine.[5]
This conspiracy of misinformation centered in part around the intentional suppression of ivermectin. A conscious disinformation campaign spearheaded by the FDA conflated human formulations of ivermectin with animal formulations. One of the tweets from the FDA’s[6 7 8 9] communications team’s “successful” “new engagement strategy,” reads: “You are not a[10] horse. You are not a cow. Seriously, y’all. Stop it.”
This “strategy” influenced medical[11] organizations, pharmacy boards, and hospitals. Their propaganda was widely cited in newspapers, magazines, digital media outlets, and medical and professional advisories. Additionally, federal and state courts began citing the posts in cases involving ivermectin, and they were referenced in legal complaints and judicial opinions across the US.[12]
This campaign was conducted with apparent malice of forethought. These acts culminated in what can only be called medical genocide. Never in recent history has a fraud of such magnitude and lethality been carried out.
Drs. Bryan Tyson and George Fareed of the United States treated 20,000 people with ivermectin, reporting 99.9 percent improvement and that none of those people went to the hospital. Dr. Shankara Chetty of South Africa reported treating 8,000 with zero mortality and 100 percent improvement. Dr. Jeff Davis of the United States reported treating 6,000 people with 100 percent improvement and zero mortality. Dr. Ben Marble of the U.S. reported treating 150,000 people with zero mortality and 99.9 percent improvement.
A case series of 39[13] physicians and their teams from around the world, all of whom used ivermectin as part of an early treatment protocol, including those physicians just mentioned, were found to have a mean improvement of over 94 percent, treating a total of 237,521 people.[14]
Dr. Mary Talley Bowden treated more than 3,900 patients for COVID-19, with a success rate of over 99.97 percent. None of the people she treated early required hospitalization. Were she and these other successful doctors celebrated? No. As a result of her success, Bowden was forced to resign her hospital privileges.[15]
The website c19early.org displays the totality of the evidence on the safety and efficacy of different early treatments, presenting real-time analysis of 3,335 studies of 56 early Covid early treatments, from a database of 5,674 treatments.
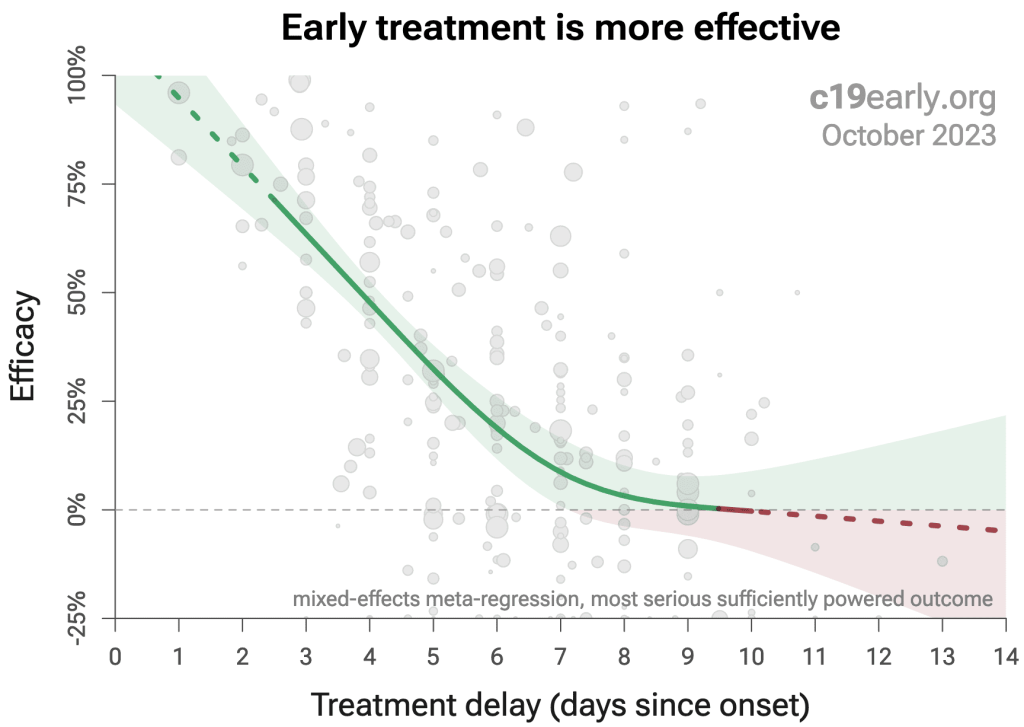
Source: c19early.org
According to this website, Ivermectin has been studied in 222 studies for Covid-19, 172 of which were peer reviewed, and 99 of which compared the treatment to a control group. These 99 studies were conducted by a total of 1089 scientists, involving 137,255 patients in 28 countries.
Ivermectin was found to be associated with statistically significant lower risk of mortality, ventilation, ICU, hospitalization and cases. Overall studies of early treatment with ivermectin show a 62 percent reduction of risk. Early treatment with ivermectin resulted in a 49 percent reduction in mortality.[16]
But instead of recommending ivermectin, the health establishment vilified it, calling it “horse dewormer.” Instead Anthony Fauci said that Gilead’s drug remdesivir would become the standard of care. According to c19early.org, remdesivir has been studied in 58 published[17] studies, conducted by a total of 946 scientists, involving 155,923 patients in 20 countries. Overall, studies of remdesivir show a 10 percent improvement. Clearly, remdesivir doesn’t[18] hold a candle to ivermectin in efficacy.
But it is more than just a question of efficacy. Ivermectin has a very high safety profile. Remdesivir, on the other hand, is consistently found to result in acute kidney failure.[19 20 21 22 23] It also appears to be dangerous if taken as a late treatment, evidence of which is presented below. None of the studies of ivermectin display risks comparable to those of remdesivir.
Sydney Wolfe of the public advocacy group Public Citizen wrote a letter to the FDA in April 2021 accusing them of improperly expediting approval for remdesivir, bypassing review by its public advisory committee. [24]
But the FDA, the CDC, the NIAID, the NIH, HHS, and their hired media partners insisted that ivermectin was dangerous and might kill you. They loudly broadcast the “news” that FDA/CDC partnered poison centers across America were fielding elevated numbers of “exposures” to ivermectin, incidentally at exactly the same time that prescriptions of ivermectin were noted anxiously by the CDC to be rising dramatically.[25]
An exposure is not a poisoning. A phone call without reported details does not itself mean[26] that it is a toxic case. The caller may have simply taken ivermectin along with five other medicines, or given animal ivermectin to his or her dog and got some on her fingers. If a person was hospitalized “after taking ivermectin,” that doesn’t mean she was hospitalized because she took ivermectin.
As far as we can determine, the basis of their propaganda[27] against ivermectin was based on a statistical hoax. In fact, we could not find evidence of a single poisoning attributable to ivermectin reported by an uncompromised, unbiased source in preparing this article. (see supplement for full analysis) On the other hand, acetaminophen, or Tylenol, is responsible for 56,000 emergency department visits, 2,600 hospitalizations, and[28 29] 500 deaths per year in the United States.[30]
Three doctors who prescribed ivermectin brought suit against the FDA and HHS and three health officials for their “horse dewormer” campaign, detailing the toll it took on their reputations and careers, such as suspensions and loss of hospital privileges. A new ruling has recently been presented on the case.
The judges ruled that the FDA’s anti-ivermectin[31] messaging stepped over the line into the realm of “practicing medicine,” which as a health agency it is not allowed to do. Its campaign against ivermectin to treat Covid-19 was not protected by its “sovereign immunity,” which shields it from being sued while carrying out its duties.
We present here the evidence that by waging an illegal propaganda war against ivermectin, the FDA, the CDC, HHS and their partners in crime were directly responsible for the wrongful deaths of 3.4 million people globally and the wrongful injuries and hospitalizations of millions or billions more. If ivermectin had not been effectively blacklisted, its use in early treatment could have saved millions of lives.
We present the peer-reviewed scientific studies from the National Library of Medicine that show that ivermectin is a safe and effective drug therapy, and could have reduced illness by up to 62 percent and mortality by 49 percent.[32]
We also present evidence that the protocols authorized for emergency use, including the kidney-toxic drug remdesivir, were deadly and never should have been considered safe or effective, as is clearly shown by the science.
Here are a few examples from the peer-reviewed literature of the benefits offered by ivermectin:
Ivermectin’s efficacy, from studies with statistically significant outcomes
- Akhtar et al found that ivermectin was significantly associated with 90 percent lower mortality, 72 percent lower ICU admission, and 80 percent higher hospital discharge.[33]
- Thairu et al found that ivermectin was significantly associated with 55 percent higher hospital discharge.[34]
- Kerr et al found that treatment with ivermectin was significantly associated with 92 percent lower mortality. In another study, the same authors found that treatment with ivermectin in[35] hospitals was significantly associated with 45 percent lower mortality. In a third study, Kerr et[36] al found that treatment with ivermectin was associated with 70 percent lower mortality, 67 percent lower hospitalization, and 44 percent fewer cases.[37]
- Ascencio–Montiel et al found that treatment with ivermectin was significantly associated with 59 percent lower mortality/hospitalization.[38]
- Shimizu et al found that ivermectin was significantly associated with 100 percent lower mortality, 48 percent lower ventilation, 43 percent lower ICU admission, 38 percent less ICU time once admitted, and 78 percent less GI complications while ventilated.[39]
- Zein et al found that people treated with ivermectin had significantly lower mortality (61 percent).[40]
- Mayer et al found that people treated with ivermectin had 55 percent lower mortality.[41]
- Samajdar et al found that people treated with ivermectin had significantly fewer cases (80 percent).[42]
Here are a few examples from the peer-reviewed literature of the dangers of late treatment with remdesivir:
- Dangers of late treatment with remdesivir, from studies with statistically significant outcomes Mitsushima et al in a retrospective analysis of 18,566 people hospitalized in Japan, found a 44 percent higher rate of mortality with late treatment using remdesivir.[43]
- Leo et al found that late treatment with remdesivir was associated with 416 percent higher disease progression.[44]
- Bowen et al found that late treatment with remdesivir was significantly associated with 57 percent higher mortality.[45]
- Alshamrani et al found that people treated late with remdesivir experienced 43 percent longer ICU admission.[46]
- Arch et al found that late treatment with remdesivir was associated with 68 percent higher ventilation.[47]
- Ohl et al found that those treated late with remdesivir had 100 percent longer hospital stays.[48]
- Schmidt et al found that late treatment with remdesivir was associated with 509 percent higher incidence of severe cases (p=.000015). [49]
- Kurniyanto et al found that late treatment with remdesivir was associated with 460 percent higher mortality (p = .0009).[50]
- Kim et al. found that late treatment with remdesivir was associated with 1612.4% higher risk of death, though the results of this study were not statistically significant.[51]
But did the results of these studies ever pass before the eyes of any of the complicit media organizations who daily recited the FDA and CDC’s official lines, completely without scientific basis though they may have been?
Thousands of media organizations parroted health agencies’ claims that the officially prescribed Covid medical interventions are safe and effective, and that ivermectin and other safe early treatments are unsafe and ineffective. The truth is just the opposite. Any of these journalists and editors could have found what we found if they had spent even two hours looking.
But they did not do that. Instead, they took orders from on high, and fell into lockstep with a tyrannical and catastrophic breakaway government. With clear malice of forethought, and by abandoning the duties of their professions, they engaged in a conspiracy against the American people, each contributing in his own way to millions of unnecessary deaths and injuries.
Intubation, Debunked Preventative Measures, EUA of Deadly mRNA Injections
The kidney-toxic remdesivir was used alongside protocols for unnecessary and lethal intubation. Most people who were intubated died. One study recorded that 76 percent of people died after intubation.[52]
Remdesivir was also used on people who were ill and weakened from dutifully following the fraudulent “preventive measures,” promoted as fervently as ivermectin was vilified. All of these have now been debunked.
They included masks, social distancing, the quarantining of healthy people and lockdowns. Ivermectin was suppressed, most importantly and most fatally, in order to clear the way for the emergency use authorization (EUA) of the mRNA gene therapy injections known as the Covid-19 “vaccines.”
These “vaccines” are a novel technology bearing no resemblance to the traditional vaccines. These mRNA injections were responsible for the injuries and death of millions of people.[53]
According to former BlackRock portfolio manager Edward Dowd and his team of PhDs and data scientists analyzing disability, actuarial and other official data sources, as of March,[54] 2023, the Covid-19 vaccines were responsible for three hundred thousand excess deaths, 26.6 million injuries, and 1.36 million disabilities. He also believes they are the cause of an 84[55] percent increase in deaths among millennials in the United States in the third quarter of 2021. [56]
The Official Death Toll: A Caveat
Altogether nearly 7 million people worldwide are estimated to have died from Covid-19. These figures are promoted forcefully and ad nauseam by the legacy media and health agencies in order to justify the narrative that Covid-19 was a health crisis of unprecedented proportions.
This narrative has been and is still being used to terrorize people, distract them, and immobilize them from rebelling at all costs and defending the few remaining threads of democratic government, civil society and the protections afforded by our Constitutional rights. Deceived by this false narrative, people became paralyzed with fear.
Then, they meekly stood by while the medical industrial complex, in coordination with captured governments and other self-interested parties, further eroded and dismantled our few remaining societal protections and democratic institutions, and ushered in a new totalitarian paradigm of bio-medical fascism and tyranny far surpassing that which existed before.
These 7 million deaths attributed to Covid must be carefully scrutinized. They have been estimated by a variety of altogether deceitful means. They cannot be trusted in any way. Most significantly, they were determined based on a fraudulent test, the PCR test, which is not a diagnostic test at all but an amplification technique designed to replicate bits of genetic material present in the system.
It cannot tell you if there is any pathogenic activity, infection or[57] disease. This fact alone simply evaporates the notion that any deaths determined by this test can be attributed to Covid-19 at all.
But with this caveat accounted for, supposing we take these official numbers of Covid deaths at face value: supposing there really were 7 million deaths from Covid-19. Ivermectin reduces risk of the most serious outcomes by 62 percent. It reduces mortality by 49 percent.
4,340,000 cases of the most serious outcomes could have been averted through the early use of ivermectin alone. 3,430,000 lives could have been saved. It is important to bear in mind that are no completely accurate statistics of how many people actually had Covid, were hospitalized or died.
How did the health authorities and the media vilify this drug? Ivermectin has a long record of safety and use. It won the Nobel Prize and was on the World Health Organization’s list of[58 59 60] essential medicines. It has been prescribed safely in humans ever since it was first marketed by Merck in 1988.
How did the health establishment convince people that this drug wasn’t the relatively safe and effective drug it has always previously been considered to be?
They engaged in a deliberate conspiracy. Through false propaganda and a marketing technique known as “informational flooding” they spread a false narrative that ivermectin was “horse[61] dewormer” and dangerous for humans to take.
They flooded the media with spurious articles promoting misleading and contradictory statistics designed to make it appear that many people were going to the hospital from ivermectin poisoning when in fact no evidence of even one poisoning, let alone one hospitalization or death, was presented by an unbiased source discoverable during the research for this article.
Then, they made it almost impossible for doctors to prescribe ivermectin to their patients by calling for a pharmacy ban on the drug. Doctors and pharmacists were intimidated by the lobby organizations for the medical industrial complex, the American Medical Association (AMA), the American Pharmacists Association (APhA) and the American Society of Health-System Pharmacists (ASHP), into acquiescing to their demands.
The AMA collects data on and maintains a full prescription history for every doctor in the United States, and would know when he or she prescribes ivermectin. Board certification organizations were threatening to[62] revoke the licenses of doctors who engaged in “misinformation and disinformation.”
They revoked the board certification or suspended the licenses of several doctors such as Meryl Nass, Pierre Kory and Paul Marik. This was to serve as an example of what other “heretical” doctors could expect to happen to them if they followed suit.[63 64 65]
This is not an isolated event in history that has been concluded and no longer poses a threat. Though the “Covid-19 pandemic” has been officially called to an end, the new architecture of “public health” and medical tyranny is ongoing and advancing, and the global framework which facilitated these atrocities can at any time be resurrected and put to fresh use. How do we stop this?
Here’s what we can prove: there was no legitimate reason for the FDA to fast-track any of the experimental vaccines under the Emergency Use Authorization policy. Because according to the FDA’s own literature, as long as there is an FDA approved drug in existence that can be used for a given disease, then you cannot have another drug or vaccine given the emergency use authorization.
However, the commercial value of marketing ivermectin or hydroxychloroquine, monocolonal antibodies, azythramyacin, vitamin C, vitamin D3, zinc and quercetin — all of which are supportive when used in combinations in stopping the spread of Covid from infection to illness and death. However, these remedies are not profitable to individuals, industries or hospitals.
Never before, as far as we are aware, has the entire machinery of federal government gone to such extreme lengths to attack, vilify and destroy a drug that has been given in billions of doses as anti-parasitic medication in humans over decades, and then to attack and vilify and cancel the reputations of mainstream highly respected physicians and scientists for using a drug successfully on their patients.
Ivermectin and these other therapies are supported by volumes in the peer-reviewed scientific literature. But the motive for destroying ivermectin and other therapies was that it was not profitable and they didn’t have control of it. This means that what they did, they did with malice and, in our opinion, unmitigated greed.
But at the time these officials made these choices, there were no counterbalancing voices in the media or governmental agencies saying, “Stop, this makes no sense. We’re talking about a medicine that clinics and physicians could use to save hundreds of thousands of lives. We should pay attention to this and do clinical studies on this.”
As a result, the man who said that he represented science, Anthony Fauci, thwarted every effort to fund a clinical study using ivermectin hydroxychloroquine, azythromyacin, monocolonal antibodies, vitamin C, vitamin D, zinc, and quercetin. But others over the next two years did do studies showing how each of these individually had statistically significant even remarkable results of saving lives.
That means that with all the outstanding resources, the very capable intelligent and skilled journalists in the media establishment could have found this information just as easily as we did. Therefore we must consider the culpability of the entire media and entire Washington health establishment as responsible for millions of preventable deaths and tens of millions of preventable hospitalizations, injuries and other suffering.
All of our footnotes and the expanded analysis offered in the technical supplement to this commentary can be used by those wanting to take this further, including class action lawsuits. They should review the information carefully.
*
Note to readers: Please click the share button above. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Richard Gale is the Executive Producer of the Progressive Radio Network and a former Senior Research Analyst in the biotechnology and genomic industries.
Dr. Gary Null is host of the nation’s longest running public radio program on alternative and nutritional health and a multi-award-winning documentary film director, including his recent Last Call to Tomorrow.
They are regular contributors to Global Research.
Notes
1 Media Partners. We Can Do This Campaign. U.S. Department of Health and Human Services. Accessed September 25, 2023. https://wecandothis.hhs.gov/sites/default/files/documents/ Paid%20Media%20List%20for%20Posting%207.12.22_508c.pdf
2 www.wecandothis.hhs.gov.
3 Celia Farber. THEY KNEW–FOIA Emails Sent To Daily Clout Team Reveal WH/CDC/NIH KNEW Covid Shots Were Causing Deadly Blood Clots And Myocarditis In MAY 2021—Senior WH Team Colluded To LIE To The American People. The Truth Barrier Substack. September 22, 2023. https://celiafarber.substack.com/p/they-knew-foia-emails- sent-to-daily
4 APTER v. DEPARTMENT OF HEALTH HUMAN SERVICES No. 22-40802 (U.S. District Court, Southern District of Texas Galveston Division, 2023). https://caselaw.findlaw.com/court/us-5th-circuit/115011736.html; No. 3:22-cv-184, June 2022 https://www.courthousenews.com/wp-content/uploads/2023/08/322cv184-three-doctors-sue-fda-over- ivermectin.pdf
5 “Globally, as of 6:32pm CEST, 27 September 2023, there have been 770,875,433 confirmed cases of COVID-19, including 6,959,316 deaths, reported to WHO. As of 19 September 2023, a total of 13,505,262,477 vaccine
doses have been administered”.WHO Coronavirus Dashboard. Accessed September 29, 2023. https:// covid19.who.int/?mapFilter=deaths
6 Why You Should Not Use Ivermectin to Treat or Prevent COVID-19. U.S. Food and Drug Administration. Content Current as of 12/10/2021. Accessed September 22, 2023. https:// www.fda.gov/consumers/consumer-updates/why-you-should-not-use-ivermectin-treat-or- prevent-covid-19
7 FAQ: COVID-19 and Ivermectin Intended for Animals. Content current as of April 26, 2021. archive.org Wayback Machine. Archived from the website of the U.S. Food and Drug Administration on December 1, 2021. https://web.archive.org/web/20211201192728/https:// www.fda.gov/animal-veterinary/product-safety-information/faq-covid-19-and-ivermectin- intended-animals?utm_medium=email&utm_source=govdelivery
8 August 21, 2021. U.S. FDA (fda): https://www.instagram.com/p/CS1giIfJ0sa/?hl=en
9 April 26, 2022. U.S. FDA (@US_FDA). https://twitter.com/US_FDA/status/ 1518942739639017472
10 APTER v. DEPARTMENT OF HEALTH HUMAN SERVICES No. 22-40802 (U.S. District Court, Southern District of Texas Galveston Division, 2023). https://caselaw.findlaw.com/court/us-5th-circuit/115011736.html; No. 3:22-cv-184, June 2022 https://www.courthousenews.com/wp-content/uploads/2023/08/322cv184-three-doctors-sue-fda-over- ivermectin.pdf
11 August 21, 2021. U.S. FDA (@US_FDA). https://twitter.com/US_FDA/status/ 1429050070243192839
12 APTER v. DEPARTMENT OF HEALTH HUMAN SERVICES No. 22-40802 (U.S. District Court, Southern District of Texas Galveston Division, 2023). https://caselaw.findlaw.com/court/us-5th- circuit/115011736.html; No. 3:22-cv-184, June 2022 https://www.courthousenews.com/wp- content/uploads/2023/08/322cv184-three-doctors-sue-fda-over-ivermectin.pdf
13 Physician Case Series Results. Version 215. August 10, 2023. Covid-19 Treatment Research. Accessed September 21, 2023. https://c19ivm.org/meta.html#fig_fpv
14 Physician Case Series Results. Version 215. August 10, 2023. Covid-19 Treatment Research. Accessed September 21, 2023. https://c19ivm.org/meta.html#fig_fpv
15 APTER v. DEPARTMENT OF HEALTH HUMAN SERVICES No. 22-40802 (U.S. District Court, Southern District of Texas Galveston Division, 2023). p. 6. https://caselaw.findlaw.com/court/us-5th-circuit/115011736.html; No. 3:22- cv-184, June 2022 https://www.courthousenews.com/wp-content/uploads/2023/08/322cv184-three-doctors-sue- fda-over-ivermectin.pdf
16 225 ivermectin COVID-19 studies, 175 peer reviewed, 99 comparing treatment and control groups. Covid-19 Treatment Research. Last accessed October 2, 2023. https://c19ivm.org/ meta.html#fig_fpv
17 Sue Hughes, Remdesivir Now ‘Standard of Care’ for COVID-19, Fauci Says, Medscape, Apr. 29, 2020, https:// www.medscape.com/viewarticle/929685 (accessed Aug. 5, 2020).
18 Remdesivir for COVID-19: real-time meta analysis of 58 studies. September 2023. Covid-19 Treatment Research. Accessed September 22, 2023. https://c19early.org/smeta.html
19 Zhou et al., Acute Kidney Injury and Drugs Prescribed for COVID-19 in Diabetes Patients: A Real-World Disproportionality Analysis, Frontiers in Pharmacology, frontiersin.org, doi.org.
20 Wu et al., Acute Kidney Injury Associated With Remdesivir: A Comprehensive Pharmacovigilance Analysis of COVID-19 Reports in FAERS, Frontiers in Pharmacology, frontiersin.org, doi.org.
21 Gérard et al., Remdesivir and Acute Renal Failure: A Potential Safety Signal From Disproportionality Analysis of the WHO Safety Database, Clinical Pharmacology & Therapeutics, wiley.com, doi.org.
22 Charan J, Kaur RJ, Bhardwaj P, Haque M, Sharma P, Misra S, Godman B. Rapid review of suspected adverse drug events due to remdesivir in the WHO database; findings and implications. Expert Rev Clin Pharmacol. 2021 Jan;14(1):95-103. doi: 10.1080/17512433.2021.1856655. Epub 2020 Dec 29. PMID: 33252992; PMCID: PMC7784780.
23 Veklury 100 mg powder for concentrate for solution for infusion remdesivir. Last revised in 01/2023. https:// www.medicines.org.uk/emc/files/pil.11597.pdf
24 https://www.trialsitenews.com/a/did-the-u-s-fda-improperly-expedite-remdesivirs-approval- the-public-citizen-demand-letter-to-fda-plus-a-trialsite-perspective
25 Rapid Increase in Ivermectin Prescriptions and Reports of Severe Illness Associated with Use of Products Containing Ivermectin to Prevent or Treat COVID-19. CDCHAN-00449. August 26, 2021. https://emergency.cdc.gov/ han/2021/han00449.asp
26 EXPOSURE VERSUS POISONING: WHAT’S THE DIFFERENCE? Washington Poison Center. Accessed September 22, 2023. https://www.wapc.org/programs/education/exposure-versus- poisoning-whats-the-difference/
27 Gustaf Kilander. Two dead from taking ivermectin in New Mexico. September 27, 2021. Independent. https:// www.independent.co.uk/news/world/americas/ivermectin-dead-new-mexico-covid-b1927767.html
28 Nourjah P, Ahmad SR, Karwoski C, Willy M. Estimates of acetaminophen (Paracetomal)- associated overdoses in the United States. Pharmacoepidemiol Drug Saf. 2006 Jun;15(6):398-405. doi: 10.1002/pds.1191. PMID: 16294364.
29 Lee WM. Acetaminophen (APAP) hepatotoxicity-Isn’t it time for APAP to go away? J Hepatol. 2017 Dec;67(6):1324-1331. doi: 10.1016/j.jhep.2017.07.005. Epub 2017 Jul 20. PMID: 28734939; PMCID: PMC5696016.
30 Agrawal S, Khazaeni B. Acetaminophen Toxicity. [Updated 2023 Jun 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https:// www.ncbi.nlm.nih.gov/books/NBK441917/
31 APTER v. DEPARTMENT OF HEALTH HUMAN SERVICES No. 22-40802 (U.S. District Court, Southern District of Texas Galveston Division, 2023). https://caselaw.findlaw.com/court/us-5th-circuit/115011736.html; No. 3:22-cv-184, June 2022 https://www.courthousenews.com/wp-content/uploads/2023/08/322cv184-three-doctors-sue-fda-over- ivermectin.pdf
32 225 ivermectin COVID-19 studies, 175 peer reviewed, 99 comparing treatment and control groups. Covid-19 Treatment Research. Last accessed October 2, 2023. https://c19ivm.org/ meta.html#fig_fpv
33 Akhtar, Tehseen & Hanif, Amber & Ali, Pyar & Haroon, Muhammad & Akram, Nimra & Raza, Muhammad & Imran, Khalid & Shakeel, Nimra & Shakeel, Ramsha. (2022). Does ivermectin reduce COVID-19 mortality and progression of disease severity? – A retrospective study.. The Professional Medical Journal. 29. 1384-1391. 10.29309/TPMJ/2022.29.09.6634.
34 Thairu, Y. & Babalola, Olufemi & Ajayi, A. & Ndanusa, Y. & Ogedengbe, John & O., Omede. (2022). A Comparison of Ivermectin and Non Ivermectin Based Regimen for COVID-19 in Abuja: Effects on Virus Clearance, Days-to-discharge and Mortality. Journal of Pharmaceutical Research International. 1-19. 10.9734/jpri/2022/v34i44A36328.
35 Kerr L, Baldi F, Lobo R, et al. (August 31, 2022) Regular Use of Ivermectin as Prophylaxis for COVID-19 Led Up to a 92% Reduction in COVID-19 Mortality Rate in a Dose-Response Manner: Results of a Prospective Observational Study of a Strictly Controlled Population of 88,012 Subjects. Cureus 14(8): e28624. doi:10.7759/cureus.28624
36 Kerr, Lucy & Baldi, Fernando & Lôbo, Raysildo & Assagra, Washington & Proença, Fernando & Hibberd, Jennifer & Chamie, Juan & Kory, Pierre & Flávio, Cadegiani. (2021). COVID-19 In- Hospital Mortality Rate is Reduced by Prophylactic Use of Ivermectin: Findings From a City- Wide, Prospective Observational Study Using Propensity Score Matching (PSM). 10.13140/ RG.2.2.26793.52327.
37 Kerr L, Cadegiani F A, Baldi F, et al. (January 15, 2022) Ivermectin Prophylaxis Used for COVID-19: A Citywide, Prospective, Observational Study of 223,128 Subjects Using Propensity Score Matching. Cureus 14(1): e21272. doi:10.7759/cureus.21272
38 Ascencio-Montiel IJ, Tomás-López JC, Álvarez-Medina V, Gil-Velázquez LE, Vega-Vega H, Vargas-Sánchez HR, Cervantes-Ocampo M, Villasís-Keever MÁ, González-Bonilla CR, Duque- Molina C. A Multimodal Strategy to Reduce the Risk of Hospitalization/death in Ambulatory Patients with COVID-19. Arch Med Res. 2022 Apr;53(3):323-328. doi: 10.1016/ j.arcmed.2022.01.002. Epub 2022 Jan 24. PMID: 35123809; PMCID: PMC8784438.
39 Shimizu K, Hirata H, Kabata D, Tokuhira N, Koide M, Ueda A, Tachino J, Shintani A, Uchiyama A, Fujino Y, Ogura H. Ivermectin administration is associated with lower gastrointestinal complications and greater ventilator-free days in ventilated patients with COVID-19: A propensity score analysis. J Infect Chemother. 2022 Apr;28(4):548-553. doi: 10.1016/j.jiac.2021.12.024. Epub 2021 Dec 31. PMID: 35016823; PMCID: PMC8718885.
40 Zein AFMZ, Sulistiyana CS, Raffaelo WM, Pranata R. Ivermectin and mortality in patients with COVID-19: A systematic review, meta-analysis, and meta-regression of randomized controlled trials. Diabetes Metab Syndr. 2021 Jul-Aug;15(4):102186. doi: 10.1016/ j.dsx.2021.102186. Epub 2021 Jun 27. PMID: 34237554; PMCID: PMC8236126.
41 Mayer MA, Krolewiecki A, Ferrero A, Bocchio M, Barbero J, Miguel M, Paladini A, Delgado C, Ojeda JR, Elorza C, Bertone A, Fleitas PE, Vera G and Kohan MR (2022) Safety and Efficacy of a MEURI Program for the Use of High Dose Ivermectin in COVID-19 Patients. Front. Public Health 10:813378. doi: 10.3389/fpubh.2022.813378
42 Samajdar SS, Mukherjee S, Mondal T, Paul J, Tripathi SK, Chakrbarty A, Saha B, Bhattacharrya D, Tripathi R. Ivermectin and Hydroxychloroquine for Chemo-Prophylaxis of COVID-19: A Questionnaire Survey of Perception and Prescribing Practice of Physicians vis-a- vis Outcomes. J Assoc Physicians India. 2021 Nov;69(11):11-12. PMID: 34781604.
43 Mitsushima S, Horiguchi H, Taniguchi K. Risk of Underlying Diseases and Effectiveness of Drugs on COVID-19 Inpatients Assessed Using Medical Claims in Japan: Retrospective Observational Study. Int J Gen Med. 2023;16:657-672. https://doi.org/10.2147/IJGM.S394413
44 Leo M, Galante A, Pagnamenta A, Ruinelli L, Ponziani FR, Gasbarrini A, De Gottardi A. Hepatocellular liver injury in hospitalized patients affected by COVID-19: Presence of different risk factors at different time points. Dig Liver Dis. 2022 May;54(5):565-571. doi: 10.1016/ j.dld.2021.12.014. Epub 2021 Dec 27. PMID: 35093272; PMCID: PMC8710398.
45 Anthony Bowen, Jason Zucker, Yanhan Shen, Simian Huang, Qiheng Yan, Medini K Annavajhala, Anne-Catrin Uhlemann, Louise Kuhn, Magdalena Sobieszczyk, Delivette Castor, Reduction in Risk of Death Among Patients Admitted With COVID-19 Between the First and Second Epidemic Waves in New York City, Open Forum Infectious Diseases, Volume 9, Issue 9, September 2022, ofac436, https://doi.org/10.1093/ofid/ofac436
46 Alshamrani AA, Assiri AM, Almohammed OA. Comprehensive evaluation of six interventions for hospitalized patients with COVID-19: A propensity score matching study. Saudi Pharm J. 2023 Apr;31(4):517-525. doi: 10.1016/j.jsps.2023.02.004. Epub 2023 Feb 15. PMID: 36819112; PMCID: PMC9930407.
47 Arch, Barbara & Kovacs, Dorottya & Scott, Janet & Jones, Ashley & Harrison, Ewen & Rosala-Hallas, Anna & Gamble, Carrol & Openshaw, Peter & Baillie, Kenneth & Semple, Malcolm. (2021). Evaluation of the effectiveness of remdesivir in treating severe COVID-19 using data from the ISARIC WHO Clinical Characterisation Protocol UK: a prospective, national cohort study. 10.1101/2021.06.18.21259072.
48 Ohl ME, Miller DR, Lund BC, et al. Association of Remdesivir Treatment With Survival and Length of Hospital Stay Among US Veterans Hospitalized With COVID-19. JAMA Netw Open. 2021;4(7):e2114741. doi:10.1001/jamanetworkopen.2021.14741
49 Schmidt AL, Tucker MD, Bakouny Z, et al. Association Between Androgen Deprivation Therapy and Mortality Among Patients With Prostate Cancer and COVID-19. JAMA Netw Open. 2021;4(11):e2134330. doi:10.1001/jamanetworkopen.2021.34330
50 Kurniyanto, Setianegari Y, Kurniaty L, Luhulima DEJ, Utomo BSR, Langi LA, Ronny, Arodes ES, Wiyanto M, Suarthana E, Wahyuningsih R. Factors associated with death and ICU referral among COVID-19 patients hospitalized in the secondary referral academic hospital in East Jakarta, Indonesia. J Clin Virol Plus. 2022 Jun;2(2):100068. doi: 10.1016/j.jcvp.2022.100068. Epub 2022 Feb 22. PMID: 35261996; PMCID: PMC8861124.
51 Kim, S.H.; Kim, T.; Choi, H.; Shin, T.R.; Sim, Y.S. Clinical Outcome and Prognosis of a Nosocomial Outbreak of COVID-19. J. Clin. Med. 2023, 12, 2279. https://doi.org/10.3390/ jcm12062279
52 Luo M, Cao S, Wei L, Zhao X, Gao F, Li S, Meng L, Wang Y. Intubation, mortality, and risk factors in critically ill Covid-19 patients: A pilot study. J Clin Anesth. 2020 Dec;67:110039. doi: 10.1016/j.jclinane.2020.110039. Epub 2020 Sep 7. PMID: 32920347; PMCID: PMC7476450.
53 Excess Mortality. 14 July 2022. Totality of the Evidence. Accessed September 20, 2023. https:// totalityofevidence.com/excess-mortality/
54 Humanity Projects: Active Projects. Phinance Technologies. Accessed September 20, 2023. https:// phinancetechnologies.com/HumanityProjects/Projects.htm#Nav_title
55 The Vaccine Damage Project – Human Cost. Phinance Technologies – Humanity Projects. Update Date: March – 2023. Phinance Technologies. Accessed September 20, 2023. https://phinancetechnologies.com/HumanityProjects/ The%20VDamage%20Project%20-%20Human%20%20Cost.htm
56 Edward Dowd. They Lied People Died. https://www.theyliedpeopledied.com/
57 Dr. Jessica Rose. Are ‘they’ trying to kill us? Unacceptable Jessica Substack. September 16, 2023. https:// jessicar.substack.com/p/are-they-trying-to-kill-us
58 Laing R, Gillan V, Devaney E. Ivermectin – Old Drug, New Tricks? Trends Parasitol. 2017 Jun;33(6):463-472. doi: 10.1016/j.pt.2017.02.004. Epub 2017 Mar 9. PMID: 28285851; PMCID: PMC5446326.
59 Thadanipon K, Anothaisintawee T, Rattanasiri S, Thakkinstian A, Attia J. Efficacy and safety of antiscabietic agents: A systematic review and network meta-analysis of randomized controlled trials. J Am Acad Dermatol. 2019 May;80(5):1435-1444. doi: 10.1016/ j.jaad.2019.01.004. Epub 2019 Jan 14. PMID: 30654070.
60 Campbell S, Soman-Faulkner K. Antiparasitic Drugs. [Updated 2023 May 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https:// www.ncbi.nlm.nih.gov/books/NBK544251/
61 Justus R. Hope M.D. The great Ivermectin deworming hoax. September 6, 2021. The Desert Review. https://www.thedesertreview.com/opinion/columnists/the-great-ivermectin- deworming-hoax/article_19b8f2a6-0f29-11ec-94c1-4725bf4978c6.html
62 Sidney M. Wolfe. The American Medical Association and Its Dubious Revenue Streams. Public Citizen Health Letter. Vol. 28. No. 11. p. 1-2. https://www.citizen.org/wp-content/ uploads/hl_201211.pdf
63 Emily Bader. Maine physician who prescribed discredited COVID treatments wanted to make a ‘spectacle’ of a state investigation. 18 months later, she said she has. The Maine Monitor. July 31, 2023. https://www.newscentermaine.com/article/news/health/meryl-nass-maine- covid-robert-f-kennedy-jr-us-fda-ivermectin/97-a611d052-b764-4f3a-be5e-cb6e5a4caad2
64 Pierre Kory. The American Board of Internal Medicine’s Longstanding War On Doctors Is Escalating. Pierre Kory’s Medial Musings. August 23, 2023. https:// pierrekorymedicalmusings.com/p/the-american-board-of-internal-medicines? utm_source=profile&utm_medium=reader2
65 Michael Nevradakis, Ph.D. Medical Board Chief Who Wanted Doctors Delicensed for ‘Misinformation’ in Bed With PR Firm Tied to CDC, Pfizer, Moderna. August 18, 2023. The Defender. Accessed September 22, 2023. https://childrenshealthdefense.org/defender/richard- baron-misinformation-weber-shandwick-conflict-of-interest-pharma-cdc/
Annex: Supplementary Materials
- Studies on ivermectin (page 7) courtesy https://c19ivm.org/
- Studies on vitamin C (page 54) courtesy https://c19early.org/c
- Studies on vitamin D3 (page 86) courtesy https://c19early.org/d
- Studies on zinc (page 198) courtesy https://c19early.org/z
- Studies on quercetin (page 242) courtesy https://c19early.org/q
- Studies on hydroxychloroquine (page 254) courtesy https://c19hcq.org
- Appendix with more detailed information and analysis about the issues mentioned in this report (page 373)
Peer-reviewed and other studies on Ivermectin
Sep 13, Liu et al., Stem Cell Research & Therapy, doi:10.1186/ s13287-023-03485-3: SARS-CoV-2 viral genes Nsp6, Nsp8, and M compromise cellular ATP levels to impair survival and function of human pluripotent stem cell-derived cardiomyocytes
In Vitro study showing that ivermectin and meclizine mitigated cardiac cell death and dysfunction caused by SARS-CoV-2 viral genes. Authors found that SARS-CoV-2 viral genes Nsp6, Nsp8, and M had harmful effects on human cardiomyocytes (h..
Aug 17, Redação MPV: Greg Tucker-Kellogg publishes fraudulent study to attack ivermectin
Discussion of errors in [medrxiv.org]. This paper is highly flawed. For example, authors claim that there were “499 reported deaths – a citywide post-hospitalisation COVID death rate of 30.1% during the study period”, whi..
Aug 10, Covid Analysis: Ivermectin for COVID-19: real-time meta analysis of 99 studies (ivmmeta)
Statistically significant lower risk is seen for mortality, ventilation, ICU admission, hospitalization, recovery, cases, and viral clearance. All remain significant for higher quality studies. 60 studies from 54 independent teams in 24..
Aug 8, Chamie et al., Cureus, doi:10.7759/ cureus.43168: COVID-19 Excess Deaths in Peru’s 25 States in 2020: Nationwide Trends, Confounding Factors, and Correlations With the Extent of Ivermectin Treatment by State
Ecological analysis showing that ivermectin distribution correlated significantly (p<0.002) with the reduction in excess deaths across 25 states in Peru. Ivermectin was authorized for COVID-19 treatment in Peru in May 2020 and distributed..
Jul 16, Osati et al., medRxiv, doi:10.1101/2023.07.13.2 3292643: Clinical manifestations and mortality among hospitalized COVID-19 patients in Tanzania, 2021-2022.
32% lower mortality (p=0.02). Retrospective 1,387 hospitalized PCR confirmed COVID-19 patients in Tanzania, showing lower mortality with ivermectin treatment and with steroid treatment in multivariable analysis.
Jul 14, Vottero et al., Molecular Sciences, doi:10.3390/ ijms241411449: Computational Prediction of the Interaction of Ivermectin with Fibrinogen
In Silico study showing that ivermectin may bind with high affinity to multiple sites on fibrinogen and may interfere with SARS-CoV-2 spike protein – fibrinogen binding, potentially inhibiting the formation of fibrin clots resistant to de..
Click here to see the full list.
*
Peer-reviewed and other studies on Vitamin C
Oct 4, Covid Analysis: Vitamin C for COVID-19: real-time meta analysis of 66 studies (64 treatment studies and 2 sufficiency studies)
Statistically significant lower risk is seen for mortality, ICU admission, hospitalization, and recovery. 22 studies from 22 independent teams in 12 countries show statistically significant improvements. • Meta analysis using the most s..
Sep 22, Seely et al., BMJ Open, doi:10.1136/ bmjopen-2023-073761: Dietary supplements to reduce symptom severity and duration in people with SARS-CoV-2: a double-blind randomised controlled trial
14% improved recovery (p=0.41). Early terminated low-risk population (no hospitalization) very late treatment (mean 8 days) RCT with 44 patients treated with vitamin C, D, K, and zinc, and 46 control patients, showing no significant differences. Authors acknowledge that..
Sep 13, Albóniga et al., Scientific Reports, doi:10.1038/ s41598-023-40999-5: Differential abundance of lipids and metabolites related to SARS-CoV-2 infection and susceptibility
Plasma metabolomic analysis showing significantly lower threonic acid levels for severe and mild COVID-19 cases compared with moderate cases. Threonic acid is a metabolite of vitamin C. The expected relationship in non-linear and depends ..