Global Prevalence and Burden of Depressive and Anxiety Disorders in 204 Countries and Territories in 2020 Due to the COVID-19 Pandemic



All Global Research articles can be read in 51 languages by activating the “Translate Website” drop down menu on the top banner of our home page (Desktop version).
To receive Global Research’s Daily Newsletter (selected articles), click here.
Visit and follow us on Instagram at @crg_globalresearch.
***
Important study on the impacts of the Covid-19 Crisis on Mental Health. Emphasis added by Global Research
Highlights
Increases in the prevalence of major depressive disorder and anxiety disorders during 2020 were both associated with increasing SARS-CoV-2 infection rates and decreasing human mobility. These two COVID-19 impact indicators incorporated the combined effects of the spread of the virus, lockdowns, stay-at-home orders, decreased public transport, school and business closures, and decreased social interactions, among other factors. We estimated that countries hit hardest by the pandemic during 2020 had the greatest increases in prevalence of these disorders.”
Summary
Background
Methods
Findings
Interpretation
Funding
*
Introduction
The emergence of the COVID-19 pandemic in 2020 against this backdrop has raised many questions around the resulting effects on mental health via its direct psychological effects and long-term economic and social consequences.4 COVID-19 continues to spread across most of the world’s populations1,2 with significant health consequences and mortality among those who become infected.5 In addition to the direct effects of COVID-19, the pandemic has created an environment in which many determinants of mental health are also affected. Social restrictions, lockdowns, school and business closures, loss of livelihood, decreases in economic activity, and shifting priorities of governments in their attempt to control COVID-19 outbreaks all have the potential to substantially affect the mental health of the population. The need for up-to-date information on the global prevalence and burden of mental disorders incorporating the mental health impacts of COVID-19 in a way that informs health system responses has never been more urgent.
Methods
Overview
First, we conducted a systematic literature review to assemble data from surveys measuring the effect of COVID-19 on the prevalence of depressive and anxiety disorders. Second, we used these data in a meta-analysis to (1) estimate the change in prevalence of major depressive disorder and anxiety disorders before versus during the COVID-19 pandemic, (2) predict (through the use of selected indicators of COVID-19 impact) the resulting change in prevalence of each disorder across all GBD locations, and (3) translate changes in prevalence to corresponding changes in burden estimates as years lived with disability (YLDs) and DALYs. A conceptual overview of this process is shown in the appendix (p 17). This study complies with the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) recommendations (appendix pp 26–27)
Case definitions
Data sources
We searched for data sources published between Jan 1, 2020, and Jan 29, 2021. The search involved electronic searches of the peer-reviewed literature using PubMed, the grey literature (ie, the COVID-19: living map of the evidence by Eppi-centre, The DEPRESSD Project, Google Scholar, The Neurology and Neuropsychiatry of COVID-19 Blog, the WHO COVID 19 literature database, COVID-Minds, and the MedRxiv and PsyArXiv preprint servers), and expert consultation. Search strings for each search are in the appendix (p 5). No language restrictions were applied.
Eligible studies reported prevalence of depressive or anxiety disorders during the COVID-19 pandemic and had a pre-pandemic baseline. We used timelines for these periods as defined by each study. Prevalence surveys conducted during the pandemic could not be included without comparable pre-pandemic data (ie, using the same instrument, location, and age group) collected since 2013 to assess the change in prevalence. Longitudinal studies using samples representative of the general population were preferred, but cross-sectional studies were also included if comparable pre-pandemic prevalence data existed. Studies using random sampling were preferred; however, due to challenges imposed by the COVID-19 pandemic, there were few studies of this type. Studies using market research quota sampling were also included but were controlled for with a covariate in our analysis. Market research quota sampling is a non-probabilistic sampling strategy whereby participants are identified from a database to match the population of interest (a discussion of the use of these estimates is in the appendix [p 7]).10 Samples obtained via this method might produce results that differ from the general population.11, 12
Studies reporting probable cases of depressive or anxiety disorders using established screening measures were included due to the paucity of available survey data from during the COVID-19 pandemic using diagnostic instruments. In these instances, only prevalence estimates for cases that reached established thresholds for probable depressive or anxiety disorder were included. We assumed the predictive validity between probable versus diagnosed cases using these screening measures did not change during the COVID-19 pandemic compared with before the pandemic, and therefore the change in the prevalence of probable cases would be equivalent to the change in the prevalence of diagnosed cases (additional discussion of this assumption is in the appendix [pp 8–9]). We also included measures capturing symptoms of both depressive and anxiety disorders (eg, the K-6 Distress Scale), which were also controlled for with a covariate in analyses. For eligible studies, we extracted information on location, age, sex, prevalence, uncertainty, number of cases, sample size, recall period, disorder, diagnostic instrument, sampling strategy, and dates between which the survey was conducted. We extracted the most detailed data reported by age and sex.
We required indicators of the impact of the COVID-19 pandemic that had an association with prevalence of major depressive disorder and anxiety disorders, hereafter referred to as COVID-19 impact indicators. The risk factor of interest was the COVID-19 pandemic, with the COVID-19 impact indicators acting as proxies for the effect of COVID-19 in the population. A COVID-19 impact indicator had to capture an effect of COVID-19, be consistently measured across locations, and be consistently measured with sufficient granularity across time (preferably daily or weekly) over the course of the pandemic. Our process of selecting the COVID-19 impact indicators is detailed in the appendix (p 10). Ultimately, we considered three novel indicators of the COVID-19 pandemic: decreasing human mobility,13 estimated total (as opposed to reported) daily SARS-CoV-2 infection rate, and estimated daily excess mortality rate during the pandemic (including excess deaths occurring during the pandemic where COVID-19 was not reported as the underlying cause of death).5, 13
The estimation of human mobility, daily SARS-CoV-2 infection rate, and daily excess mortality rate was done by the Institute for Health Metrics and Evaluation (IHME) COVID-19 Forecasting Team and is described in detail elsewhere.13 In summary, human mobility was represented by a composite human mobility index representing daily change from pre-pandemic mobility. Data from mobile phone users provided by Facebook, Google, Descartes Labs, Safegraph, and Baidu, and data on physical distancing mandates informed a Gaussian process regression to estimate a time series for human mobility. Daily SARS-CoV-2 infection and excess mortality rates were estimated via a deterministic susceptible, exposed, infectious, and recovered (known as SEIR) compartmental framework and was informed by daily confirmed SARS-CoV-2 infections, COVID-19-related deaths, SARS-CoV-2 tests conducted, antibody seroprevalence, human mobility, physical distancing mandates, pneumonia seasonality, facemask use, and vaccine coverage.5, 13
GBD conducts routine systematic reviews of the epidemiology of major depressive disorder and anxiety disorders as part of the estimation of YLDs (and separately to the aforementioned systematic review of the change in prevalence due to COVID-19). The compiled epidemiological data for GBD 2020 includes studies done from 1980 to 2019 on the prevalence, incidence, remission, duration, and excess mortality of major depressive disorder and anxiety disorders. These data were identified through routine electronic searches of PubMed, PsycINFO, Embase, grey literature sources (including a review of the Global Health Data Exchange library), and consultation with experts. GBD 2020 uses Disease Modelling Meta-Regression version 2.1 (known as DisMod-MR 2.1), a Bayesian disease modelling meta-regression tool, to analyse these data and generate internally consistent estimates of prevalence, incidence, remission, and mortality by sex, location, year, and age group for each disorder.
14 It also estimates prevalence for locations that are missing raw epidemiological data. GBD 2020 does this by estimating prevalence across a cascade down five levels of a geographical hierarchy: global, super-region, region, country or territory, and subnational locations. The prevalence from locations higher in the hierarchy act as priors for the prevalence for locations lower in the hierarchy. More detail on DisMod-MR 2.1 and the estimation of prevalence data for major depressive disorder and anxiety disorders has been published elsewhere.1, 14 Because no epidemiological data from the year 2020 informed the DisMod-MR 2.1 model for major depressive disorder and anxiety disorders, the prevalence produced for 2020 by age and sex and for each of the 204 countries and territories represented the prevalence of each disorder without the impact of the COVID-19 pandemic.
We made use of severity distributions and disability weights in GBD 2020 (appendix p 32). We apportioned the final disorder prevalence for the year 2020 into the categories of asymptomatic, mild, moderate, and severe with corresponding disability weights. Disability weights in GBD 2020 quantify health loss from a health state on a scale of 0 (no health loss) to 1 (equivalent to death). The process to estimate severity proportions and disability weights in GBD 2020 has been described elsewhere.2,15
Statistical analysis
Due to the strong collinearity between the COVID-19 impact indicators (inspected via Pearson correlation coefficients) and the need for age, sex, and bias covariates to be treated as effect modifiers on the impact indicators, we developed prevalence adjustment models via a two-step process. In step one, we used indicator models to develop a so-called index for the impact of COVID-19. Human mobility, daily SARS-CoV-2 infection rate, and daily excess mortality rate were included simultaneously in a meta-regression on the change in logit prevalence to quantify their independent effect on prevalence change. We used the coefficients from these models to calculate a single COVID-19 impact indicator for each disorder. In step two, we developed a final model for each disorder via backward elimination to regress the COVID-19 impact indicator, age, sex, and the bias covariates on the change in logit prevalence. The least significant covariate was iteratively removed until no improvement was seen in the Akaike information criterion. We assessed the generalisability of the model using a leave-one-country-out cross-validation analysis (appendix p 11).
Consistent with GBD methods, we followed ICD rules for determining the underlying cause of death. DALYs for major depressive disorder and anxiety disorders were composed entirely of YLDs, which meant that, despite potential excess deaths, major depressive disorder and anxiety disorders were not considered underlying causes of death.2 We first estimated sequela-specific YLDs by multiplying sequela-specific prevalences by their respective disability weights. We then corrected the sequela-specific YLDs for comorbidities to adjust for the co-occurrence of causes of YLDs within GBD 2020; these methods have been described in detail elsewhere.1 For GBD 2020, burden is only estimated using the COVID-19-adjusted prevalence estimates. Therefore, we calculated baseline burden estimates by adjusting GBD 2020 burden estimates by the ratio between baseline prevalence and adjusted prevalence.
p values of less than 0.05 were considered to be significant. We did all analyses using DisMod MR-2.1, MR-BRT, and R (version 3.6.3).
Role of the funding source
Results
Human mobility and daily SARS-CoV-2 infection rate were significantly associated with the change in major depressive disorder and anxiety disorder prevalence (table 1). After controlling for human mobility and daily SARS-CoV-2 infection rate, daily excess mortality rate was not associated with the change in prevalence for either major depressive disorder or anxiety disorders. This was likely due to high collinearity between the daily excess mortality rate and the other two COVID-19 impact variables (r = 0·8 with daily SARS-CoV-2 infection rate and r = 0·8 with human mobility), which was less of an issue shared between the daily SARS-CoV-2 infection rate and human mobility (r = 0·5).
Table 1. Meta-regression coefficients from the indicator model on the change in major depressive disorder and anxiety disorders logit prevalences over the course of the COVID-19 pandemic in 2020
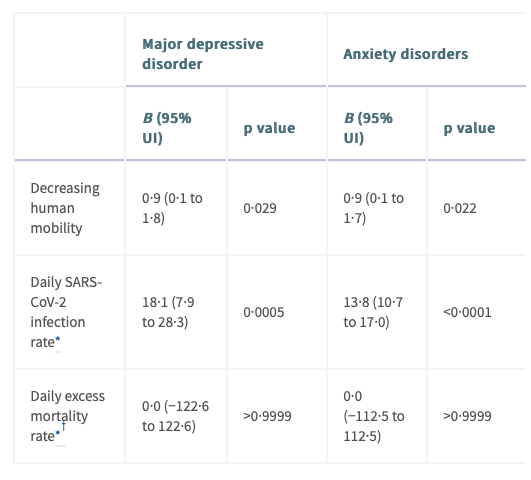
All indicators included in the model simultaneously and therefore control for each other. UI=uncertainty interval.
* Square-root transformed before analysis to correct for positive skew appendix pp 6–7.
† Bayesian directional prior specified due to strong collinearity with other indicators.
Table 2. Meta-regression coefficients on the change in major depressive disorder and anxiety disorders logit prevalences over the course of the COVID-19 pandemic in 2020
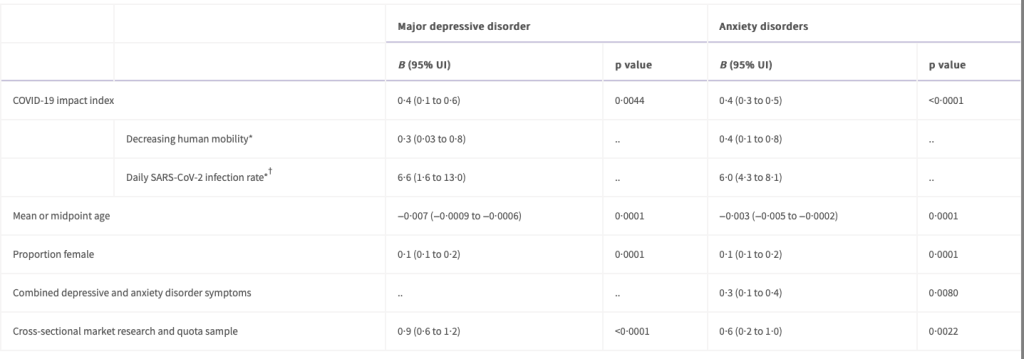
Longitudinal market research and quota sample was not significant, and so not included in the final model.
* Coefficients are estimated using the B of the COVID-19 impact index multiplied by the B of the COVID-19 impact indicators from the signal model and 95% UIs estimated via multiplying 1000 samples of the posterior distribution of these impact indicator covariates from the indicator model with 1000 samples of the posterior distribution of the indicator coefficient.
† Square-root transformed before analysis to correct for positive skew of the COVID-19 impact index coefficient appendix pp 6–7. UI=uncertainty interval.
Before adjustment for the COVID-19 pandemic, the estimated global prevalence of major depressive disorder in 2020 was 2470·5 cases (95% UI 2143·5–2870·7) per 100 000 population, equivalent to 193 million (167–224) people (appendix pp 35–50). After adjustment for the COVID-19 pandemic, the estimated prevalence of major depressive disorder was 3152·9 cases (2722·5–3654·5) per 100 000 population, equivalent to 246 million (212–285) people. We estimated an additional 53·2 million (44·8–62·9) cases of major depressive disorder globally in 2020 due to the effects of COVID-19 (682·4 [574·1–807·2] new cases per 100 000 population, an increase of 27·6% [25·1–30·3]; table 3). Females had a greater increase in prevalence of major depressive disorder than males did, with 35·5 million (30·0–41·8) additional cases among females (equivalent to 912·5 [772·1–1075·2] per 100 000 females; a 29·8% [27·3–32·5] increase) compared with 17·7 million (14·7–21·3) additional cases in males (equivalent to 453·6 [376·3–545·0] per 100 000 males; a 24·0% [21·5–26·7] increase; data by sex by super-region and region are available on the Global Health Data Exchange). Global patterns of prevalence before and after adjustment for (ie, during) the COVID-19 pandemic, by age and sex, are presented in figure 1, and estimates of the change in prevalence of major depressive disorder are shown in figure 2 and in the appendix (p 21).
Table 3. Prevalence of major depressive disorder and anxiety disorders, by super-region, 2020
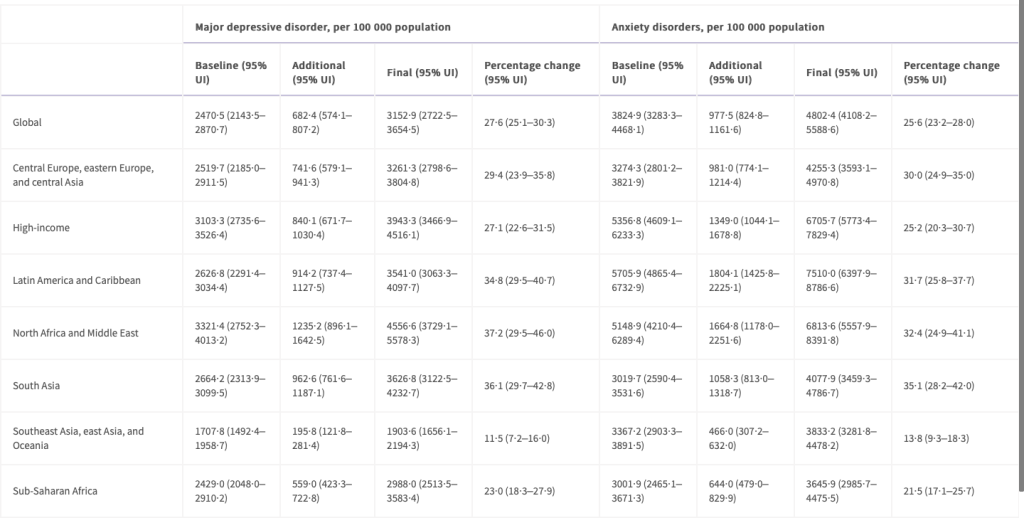
UI=uncertainty interval.
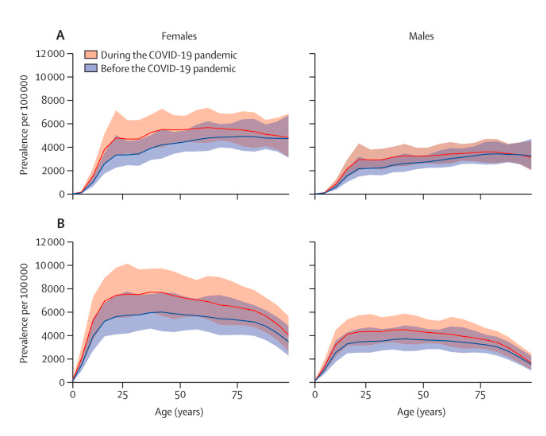
Figure 1. Global prevalence of major depressive disorder (A) and anxiety disorders (B) before and after adjustment for (ie, during) the COVID-19 pandemic, 2020, by age and sex
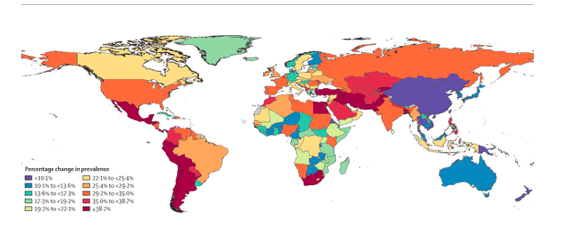
Figure 2. Change in the prevalence of major depressive disorder after adjustment for (ie, during) the COVID−19 pandemic, 2020
Before adjustment for the COVID-19 pandemic, the estimated global prevalence of anxiety disorders in 2020 was 3824·9 (95% UI 3283·3–4468·1) per 100 000 population, which is equivalent to 298 million (256–348) people (appendix pp 51–66). After adjustment for the COVID-19 pandemic, the global prevalence of anxiety disorders in 2020 was 4802·4 (4108·2–5588·6), equivalent to 374 million (320–436) people. We estimated an additional 76·2 million (64·3–90·6) cases of anxiety disorders in 2020 due to the COVID-19 pandemic (977·5 [824·8–1161·6] new cases per 100 000 population; an increase of 25·6% (23·2–28·0) globally (table 3). Females had a greater increase in prevalence than males did, with 51·8 million (43·8–61·1) additional cases among females (equivalent to 1332·1 [1126·1–1573·2] per 100 000 females; a 27·9% [25·6–30·4] increase) compared with 24·4 million (20·3–29·5) additional cases among males (equivalent to 625·0 [518·3–755·3] per 100 000 males; a 21·7% [19·3–24·1] increase; data by sex by super-region and region will be available on the Global Health Data Exchange after full release of GBD 2020). Global patterns of prevalence before and after adjustment for (ie, during) the COVID-19 pandemic, by age and sex, are presented in figure 1, and estimates of the change in prevalence of anxiety disorders are shown in figure 3 and in the appendix (p 22).
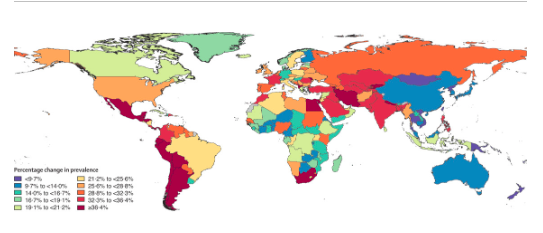
Figure 3. Change in the prevalence of anxiety disorders after adjustment for (ie, during) the COVID−19 pandemic, 2020
Before adjustment for the COVID-19 pandemic, major depressive disorder was responsible for 38·7 million (95% UI 26·4–53·9) DALYs globally, equivalent to 497·0 DALYs (338·3–691·1) per 100 000 population. After adjustment for the COVID-19 pandemic, major depressive disorder was responsible for 49·4 million (33·6–68·7) DALYs, equivalent to 634·1 DALYs (431·3–881·0) per 100 000 population (appendix pp 35–50). We estimated that the COVID-19 pandemic led to an additional 10·7 million (7·21–14·9) DALYs for major depressive disorder globally, of which 7·07 million (4·80–9·80) were among females and 3·62 million (2·40–5·09) were among males. The global major depressive disorder additional DALY rate due to the COVID-19 pandemic was 137·1 DALYs (92·5–190·6) per 100 000 population, 182·0 (123·5–252·2) per 100 000 females, and 92·5 (61·5–130·3) per 100 000 males (DALY rates by sex by region will be available on the Global Health Data Exchange after full release of GBD 2020). The burden of DALYS due to major depressive disorder by age and sex is presented in figure 4.

Figure 4. Global burden of major depressive disorder and anxiety disorders by age and sex, 2020
Before adjustment for the COVID-19 pandemic, anxiety disorders were responsible for 35·5 million (95% UI 23·9–50·1) DALYs globally, equivalent to 454·8 DALYs (307·0–642·5) per 100 000 population (appendix pp 51–66). After adjustment for the COVID-19 pandemic, anxiety disorders were responsible for 44·5 million (30·2–62·5) DALYs globally, equivalent to 570·9 (387·3–802·2) per 100 000 population. Anxiety disorders were responsible for an additional 9·05 million (6·18–12·8) DALYs due to the pandemic, of which 6·11 million (4·21–8·56) DALYs were among females and 2·94 million (1·97–4·19) among males. The global anxiety disorder additional DALY rate due to the COVID-19 pandemic was 116·1 (79·3–163·8) per 100 000 population, 157·2 (108·3–220·3) per 100 000 females, and 75·3 (50·3–107·1) per 100 000 males. The burden of DALYS due to anxiety disorders by age and sex is presented in figure 4.
Discussion
Increases in the prevalence of major depressive disorder and anxiety disorders during 2020 were both associated with increasing SARS-CoV-2 infection rates and decreasing human mobility. These two COVID-19 impact indicators incorporated the combined effects of the spread of the virus, lockdowns, stay-at-home orders, decreased public transport, school and business closures, and decreased social interactions, among other factors. We estimated that countries hit hardest by the pandemic during 2020 had the greatest increases in prevalence of these disorders.
The two COVID-19 impact indicators used in our model should not be interpreted as risk factors for major depressive disorder and anxiety disorders. The risk factor of interest was the COVID-19 pandemic, with these two indicators acting as proxies for the effect of COVID-19 in the population. The COVID-19 pandemic is occurring against a complex backdrop of a range of social determinants of mental health, as well as well known inequalities within these determinants. The greater increase in disorder prevalence among females than among males, which resulted in an even greater sex difference in prevalence than before the pandemic, was anticipated because females are more likely to be affected by the social and economic consequences of the pandemic.17, 18, 19 Additional carer and household responsibilities due to school closures or family members becoming unwell are more likely to fall on women.17 Women are more likely to be financially disadvantaged during the pandemic due to lower salaries, less savings, and less secure employment than their male counterparts.17, 18, 19 They are also more likely to be victims of domestic violence, the prevalence of which increased during periods of lockdown and stay-at-home orders.20, 21 We also estimated greater change in the prevalence of major depressive disorder and anxiety disorders among younger age groups than among older age groups. UNESCO declared COVID-19 to be the most severe disruption to global education in history, estimating 1·6 billion learners in over 190 countries to be fully or partially out of school in 2020.22 With school closures and wider social restrictions in place, young people have been unable to come together in physical spaces, affecting their ability to learn and for peer interaction. Furthermore, young people are more likely to become unemployed during and following economic crises than older people.23
Our study is not the first to show how population shocks (ie, unexpected or unpredictable events that disrupt the environmental, health, economic, or social circumstances within a population) can increase the prevalence of depressive and anxiety disorders. In their review of mental health outcomes after the economic crisis in 2009, Frasquilho and colleagues24 identified several studies showing an increase in common mental disorders in the general population. After the 2009 financial crisis in Greece, point prevalence of major depressive episodes increased from 3·3% (95% UI 3·1–3·5) in 2008 to 6·8% (6·4–7·2) in 2009 and 8·2% (8·1–8·3) in 2011.25 Survey respondents reporting serious economic hardship were most at risk of developing a major depressive episode.25, 26 Similarly, after the 2008 financial crisis in Hong Kong, past-year prevalence of major depressive episodes increased from 8·2% (95% UI 7·2–9·2) in 2007 to 12·5% (11·0–13·9) in 2009.27 The extent of the increase in prevalence differed across studies, which might be due to study or population characteristics or different combinations of health and socioeconomic determinants of poor mental health, or a combination of these factors. Another point of difference is the time period over which the impact of the shock is measured. This period might be a single point in time, weeks or months, or, as in our analysis, an average over the course of a longer period (eg, a year) during which there would have been fluctuating effects from the pandemic (ie, the shock).
Both major depressive disorder and anxiety disorders increase the risk of other diseases and suicide.28, 29 In their time-series analysis of the impact of COVID-19 on suicide rates across 21 high-income and middle-income countries, Pirkis and colleagues30 found no significant increases in suicide rates between April and July, 2020. This finding raises the question of whether or not the increased prevalence of major depressive disorder and anxiety disorders we found was accompanied by a significant increase in suicide rates. We have insufficient data to draw any conclusions on this matter. Pirkis and colleagues30 relied on data in the first few months of the pandemic, which might have been too early in the pandemic to detect an association between a new diagnosis of major depressive disorder or anxiety disorders and suicide. Suicide trends might vary over extended periods, and as we progress through different phases of the pandemic the full scale of economic consequences and their effects will emerge, and their subsequent effects on suicide trends. For example, Tanaka and Okamota31 found that, although suicide rates in Japan decreased by 14% during the first 5 months of the pandemic (February to June, 2020), they then increased by 16% (between July and October, 2020), with a larger increase among females and younger populations than among males and older populations.
Contributors
COVID-19 Mental Disorders Collaborators
Affiliations
*
Note to readers: Please click the share buttons above or below. Follow us on Instagram, @crg_globalresearch. Forward this article to your email lists. Crosspost on your blog site, internet forums. etc.
Notes
1. GBD 2019 Disease and Injuries Collaborators
Lancet. 2020; 396: 1204-1222
2. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of mental disorders in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet Psychiatry (in press).
3. Patel V, Chisholm D, Parikh R, et al.
Lancet. 2016; 387: 1672-1685
4. Kola L, Kohrt BA, Hanlon C, et al.
Lancet Psychiatry. 2021; 8: 535-550
5. Institute for Health Metrics and Evaluation COVID-19 projections.
Institute for Health Metrics and Evaluation, University of Washington, Seattle, WA2020
https://covid19.healthdata.org/
Date accessed: September 28, 2021
6. Stevens GA, Alkema L, Black RE, et al.
PLoS Med. 2016; 13e1002056
7. American Psychiatric Association
4th edn, text revised. American Psychiatric Association,Washington, DC2000
8. WHO
World Health Organization, Geneva1992
9. Page MJ, McKenzie JE, Bossuyt PM, et al.
BMJ. 2021; 372: n71
10. Lavrakas PJ
in: Encyclopedia of survey research methods. Sage Publications,Thousand Oaks, CA2008
11. Heen M, Lieberman J, Miethe T
UNLV Center for Crime and Justice Policy, 2014
https://www.unlv.edu/sites/default/files/page_files/27/ComparisonDifferentOnlineSampling.pdf
Date accessed: September 14, 2021
12. Levay KE, Freese J, Druckman JN
SAGE Open. 2016; 6 (2158244016636433)
13. Institute for Health Metrics and Evaluation COVID-19 Forecasting Team
Nat Med. 2021; 27: 94-105
14. Flaxman AD, Vos T, Murray CJL
1st edn. University of Washington Press, Seattle, WA2015
15. Burstein R, Fleming T, Haagsma J, Salomon JA, Vos T, Murray CJL
Popul Health Metr. 2015; 13: 31
16. Zheng P, Barber R, Sorensen RJD, Murray CJL, Aravkin AY
J Comput Graph Stat. 2021; (published online Feb 12.)
17. UN
United Nations, April 9, 2020
18. Wenham C, Smith J, Davies SE, et al.
Nature. 2020; 583: 194-198
19. Burki T
Lancet Infect Dis. 2020; 20: 904-905
20. Piquero AR, Jennings WG, Jemison E, Kaukinen C, Knaul FM
J Crim Justice. 2021; 74101806
21. Arenas-Arroyo E, Fernandez-Kranz D, Nollenberger N
J Public Econ. 2021; 194104350
22. UNESCO
UNESCO, 2021
Date accessed: April 21, 2021
23. Bell DNF, Blanchflower DG
Oxf Rev Econ Policy. 2011; 27: 241-267
24. Frasquilho D, Matos MG, Salonna F, et al.
BMC Public Health. 2016; 16: 115
25. Economou M, Madianos M, Peppou LE, Patelakis A, Stefanis CN
J Affect Disord. 2013; 145: 308-314
26. Madianos M, Economou M, Alexiou T, Stefanis C
Soc Psychiatry Psychiatr Epidemiol. 2011; 46: 943-952
27. Lee S, Guo WJ, Tsang A, et al.
J Affect Disord. 2010; 126: 125-133
28. Clarke DM, Currie KC
Med J Aust. 2009; 190: S54-S60
29. Moitra M, Santomauro D, Degenhardt L, et al.
J Psychiatr Res. 2021; 137: 242-249
30. Pirkis J, John A, Shin S, et al.
Lancet Psychiatry. 2021; 8: 579-588
31. Tanaka T, Okamoto S
Nat Hum Behav. 2021; 5: 229-238
32. Jorm AF, Patten SB, Brugha TS, Mojtabai R
World Psychiatry. 2017; 16: 90-99
33. Thornicroft G
Lancet. 2007; 370: 807-808
34. Maulik PK, Thornicroft G, Saxena S
Int J Ment Health Syst. 2020; 14: 57
35. Campion J, Javed A, Sartorius N, Marmot M
Lancet Psychiatry. 2020; 7: 657-659
36. Moreno C, Wykes T, Galderisi S, et al.
Lancet Psychiatry. 2020; 7: 813-824
37. Huang C, Huang L, Wang Y, et al.
Lancet. 2021; 397: 220-232
38. Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ
Lancet Psychiatry. 2021; 8: 416-427
39. Winkler P, Formanek T, Mlada K, et al.
Epidemiol Psychiatr Sci. 2020; 29: e173
40. Ayuso-Mateos JL, Morillo D, Haro JM, Olaya B, Lara E, Miret M
Epidemiol Psychiatr Sci. 2021; 30: e49
41. Knudsen AKS, Stene-Larsen K, Gustavson K, et al.
Lancet Reg Health Eur. 2021; 4100071
42. Solmi F, Downs JL, Nicholls DE
Lancet Child Adolesc Health. 2021; 5: 316-318