

All Global Research articles can be read in 51 languages by activating the Translate Website button below the author’s name.
To receive Global Research’s Daily Newsletter (selected articles), click here.
Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
***
Iron and copper are highly interdependent and need to be considered together. Low ferritin is rarely indicative of low iron. In most cases, it’s a sign that copper insufficiency is preventing proper iron recycling
Copper deficiency will down-regulate several genes, including aldose reductase-1 (which plays a crucial role in glucose and fructose metabolism), glutathione peroxidase (a master antioxidant enzyme), mitochondrial aconitase (involved in iron metabolism in the mitochondria) and transferrin (which mediates the transport of iron)
Iron deficiency virtually doesn’t exist outside of acute blood loss that is unrelated to menstruation. Unless you have a history of acute blood loss, you are likely dealing with iron recycling dysfunction due to copper deficiency
The best way to lower excessive iron is to donate blood. Most adult men and postmenopausal women have high iron and could benefit from regular blood donation, as high iron is extremely toxic and destroys health
To raise your copper level, you could use a copper bisglycinate supplement, or foods like grass fed beef liver, bee pollen and whole food vitamin C
*
Here, I interview repeat guest Morley Robbins, MBA, CHC,1 founder of the Magnesium Advocacy Group and author of “Cu-RE Your Fatigue: The Root Cause and How to Fix It on Your Own.”
While we’ve discussed the topic of iron and copper before, the percentage of doctors and natural medical clinicians who understand his work is probably about 1% or less, so it’s well worth revisiting. Besides, it’s near-impossible to learn this information in a single interview without repeated review of these vital principles.
Iron is often viewed as a universal panacea that most need more of, but nothing could be further from the truth. The reality is that almost everyone, with the exception of menstruating women, or those with large blood losses, have too much iron.
Conversely, copper is often considered toxic, yet most people are deficient and actually need more in order for their iron metabolism to function properly. Without copper, your iron will not recycle properly, resulting in what appears to be a low iron level upon testing.
The real problem, however, is not low iron but low copper. Adding iron will only worsen the situation as excess iron is extremely damaging to your cardiovascular system. Iron rusts, and that’s basically what happens in your blood vessels as well.
Effects of Copper Deficiency
Robbins cites animal research2 from 2009 that looked at what happens to genes (which are responsible for encoding proteins) when rats are denied copper. As it turns out, six genes (and subsequent proteins) are down-regulated or turned off, while one gene in particular, transferrin, is upregulated, as follows:
- Beta-enolase (ENO3)
- Carbonic anhydrase, which increases carbon dioxide access, assisting rapid inter-conversion of carbon dioxide and water into carbonic acid, protons and bicarbonate ions. Carbonic anhydrase is billed as a zinc enzyme but it’s actually a copper enzyme
- Aldose reductase-1, which plays a crucial role in glucose and fructose metabolism
- Glutathione peroxidase (GPX), one of your master antioxidant enzymes, which is copper dependent
- Muscle creatine kinase, which your muscles need to function as it plays an important role in energy production
- Mitochondrial aconitase, which is involved in iron metabolism in the mitochondria
- Transferrin, which binds to and mediates the transport of iron through blood plasma, is upregulated, among others, in a state of copper deficiency
If you’re copper deficient, none of these genes will function properly, and beyond these, there are at least 300 other genes that are also copper-dependent. Your mitochondria also need copper for optimal function, and mitochondrial dysfunction is a driver of virtually all chronic disease and ill health.
The Importance of Copper for Mitochondrial Function
Copper and its master protein, ceruloplasmin, are instrumental for mitochondrial function. Ceruloplasmin is what drives the copper into the mitochondria, and each mitochondrion needs about 50,000 atoms of copper to do its work.
There are five cytochrome complexes embedded in your inner mitochondrial membranes. Their purpose is to shuttle electrons created from the food you eat that is ultimately converted to acetyl-CoA to produce ATP. If these complexes are deficient in key minerals you will not be able to generate enough cellular energy.
The enzymes of the mitochondrial respiratory chain are called mitochondrial respiratory complexes. Complexes 1, 3, 4 and 5 are copper-dependent. Complexes 1, 3 and 4 create what is called “the respirasome,” and they work together as a unit to stimulate NADH dehydrogenase activity. (NADH dehydrogenase is an enzyme that converts NAD from its reduced form, NADH, into its oxidized form NAD+, which is important for mitochondrial function and healthy muscle mass.)
Complexes 1, 3, 4 (acting as the respirasome) are hooked up to cardiolipin, a unique fat found only in the mitochondrial membrane that supports copper and enables the dynamics of the electron transport to take place. Retinol (vitamin A) is also crucial for moving electrons from complex 3 to complex 4.
The Type of Fat You Eat Matters
Now, the composition of fatty acids, such as cardiolipin, is completely dependent on what you are eating. If you’re like most Americans and 20% to 30% of the fat you eat is omega-6 linoleic acid, a high percentage of the fatty acids in the cardiolipin is going to consist of linoleic acid. If you eat a lot of saturated fat, or mono-unsaturated fat, then it’s going to be made up of that.
Why is that important? Because unsaturated fats like linoleic acid are predisposed to oxidation. And when you have oxidation in cardiolipin, you are destroying the structure of your mitochondria and decimating the ability of the mitochondria to function well. They can’t transfer electrons as efficiently when cardiolipin is oxidized.
The only place cardiolipin is found in your body is in the cristae of your inner mitochondrial membrane of your mitochondria. This is where most of your cytochrome complexes are embedded. If cardiolipin is damaged then the complexes will not be close together to form supercomplexes and thus they will not be able to generate as much mitochondrial energy. It’s also important to know what the match causing the oxidation is, and that’s iron.
“When people are told they have low iron in the blood, the practitioner doesn’t know that iron is high in the tissue, and then they give them more iron, and what’s the iron going to do? It’s going to find its way to the cell, and then it’s going to find its way to the mitochondria, and then, there’s this collapse in energy production,” Robbins explains.
Understanding Iron Testing
The confusion that pervades the iron issue is how to actually measure it. Seventy percent of the iron in your body is stored in the hemoglobin in your red blood cells, 10% is found in intercellular protein, and only one-tenth of 1% of the iron is serum iron, attached to transferrin.
The key detail here is that your red blood cells are not in your blood but actually float in the watery serum portion of the blood that gets measured when you do a blood test. So, when you’re measuring serum ferritin, you are not actually getting a true measure of your iron stores. Low ferritin is typically interpreted as low iron, but that is a major clinical mistake.
You need to look at all of the containers of iron — hemoglobin, serum iron and ferritin. You also need to look at non-iron markers such as zinc, copper and ceruloplasmin, as well as vitamin A and vitamin D because they influence the bioavailability of copper. This holistic evaluation is the focus of Robbins’ “Root Cause” protocol.
What’s the Problem if You Have Low Ferritin?
According to Robbins, when someone is told they have low iron because their ferritin is low, 99.9% of the time the real problem is iron recycling dysfunction related to copper deficiency. This contradicts almost every medical “expert” in the world, so it’s a major claim, but understanding it can have a significant impact on your health.
Basically, “iron deficiency” virtually doesn’t exist outside of acute blood loss that is unrelated to menstruation. Unless you have a history of acute blood loss, say due to an injury, you are likely dealing with iron recycling dysfunction due to copper deficiency.
“We have the myth of iron deficiency. We have the myth that iron regulates itself. It does not. It is entirely copper dependent. When you get into the real deep research, you’re going to find that copper is the General, iron is the foot soldier. Now try to picture the Battle of the Bulge without Patton. Very different story there.
The third is this idea that, ‘Well I feel so much better when I take iron.’ Dr. Robert E. Hodges in 1978 did a masterful job of explaining the deception of iron supplementation. It offers a six-week hit. Hemoglobin does go up, people are going to feel a little bit better. But it’s only going to last for six weeks.
He was able to document it meticulously in the three-year study that he did with humans. He was able to show exactly why they respond. The key is that any heavy metal, and iron is a heavy metal … is going to force increased red blood cells. There is this dynamic of heavy metals driving more red blood cells, [likely] to deliver more oxygen to deal with the toxicity.
But the increase of iron and the feeling better is short-lived and deceptive. When did all of the blood marker dynamics change in Dr. Hodge’s study? When he introduced retinol, which makes copper bioavailable.”
High Ferritin Is Often a Sign of Liver Dysfunction
On the flip-side we have high ferritin. This is routinely interpreted as having normal (or high) iron stores, but that’s not accurate either. Importantly, when you have high ferritin, it’s oftentimes a sign of liver dysfunction. The ferritin is spilling out of the liver into the bloodstream because the recycling center of the hepatocyte is not working.
The liver’s recycling center is called the lysosome. This is where ferritin is turned over to make iron available for use. When that lysosome isn’t working right, iron will accumulate in the liver, causing ferritin to be secreted into the cell. The key to proper iron recycling in the liver is, again, copper. The loading of iron in ferritin that takes place inside the cell, and the recycling of ferritin inside the cell, is entirely copper-dependent. Robbins explains:
“Copper goes into the ferritin as a result of ferroxidase enzyme function, which is copper driven. And then, copper is needed to recycle that ferritin protein, break it down and let the iron out. It’s a copper-dependent process.
People don’t realize the role that copper chaperones are playing to move that iron where it’s needed in the body. And the principle chaperone for iron in the blood, the serum iron, is transferrin.”
As mentioned earlier, the gene that encodes transferrin is upregulated when copper is deficient. So, transferrin rises counterintuitively, due to copper insufficiency, iron gets sequestered into the RES macrophages, and thus iron is not recycled and distributed properly. Robbins continues:
“There was a different [study in which] they were using rodents, denying [them] copper. They were looking at 13 different genes. The only gene that fired up in the face of copper deficiency was the ferritin light chain (FTL) gene. It’s very different than ferritin heavy chain (FTH), which is copper-dependent, because it, again, relies on the ferroxidase enzyme.
And where is ferritin light chain found? It’s found in the liver, and iron builds up in the liver in a copper-deficient body. We’ve known that since 1928 … (Hart et al., 1928)
I think what’s important, the big macro for everyone in this conversation, is to see the profound interaction that copper and iron have in our metabolism, and that there is no iron metabolism, there’s only copper-iron metabolism, and you can’t make conclusions on iron status, by measuring just serum ferritin status.”
How Much Iron Do You Need?
As mentioned, unless you’re losing a lot of blood, your iron will (most likely) be high. The reason for this is because your body has no way of eliminating iron, other than blood loss.
High iron, due to its corrosive nature, can cause tremendous damage inside your body. You only need 25 milligrams of iron in your body for red blood cell maintenance, and 24 of those 25 mg come from the recycling system (provided you have enough copper to make it work as it should).
So, you need very little iron from your diet — only 1 mg per day. The problem is that the optimal amount of iron needed is about 5,000 mg. Older people can have closer to 25,000 or 30,000 mg, thanks to excessive intake over the course of their lives.
“What’s happening is there’s total silence about iron recycling,” Robbins says. “Because we live in this copper deficient environment, the recycling system is not as efficient. The serum iron is going to show low under those conditions. The doctor is going to react with, ‘You need more iron,’ when in fact what you need is more copper. The recycling system is dependent upon one iron egress doorway.
It’s called ferroportin (iron doorway) and ferroportin entirely depends on a copper enzyme. It’s called hephaestin. It’s a copper protein that expresses the exact same enzyme as ceruloplasmin, called ferroxidase.
What hephaestin does is make sure that the iron gets out of the recycling macrophages as soon as possible — 2.5 times faster than if copper’s not present — and ensures it’s loaded onto transferrin to take that iron to the bone marrow [where red blood cells are created 2.5 million times per second].
That recycling system that’s occurring all day and all night is never factored into the clinician’s interpretation of blood work. They’re just seeing low numbers and they’re not thinking recycling, they’re only thinking replacement.
I think that would be a really important takeaway for people — to question your doctor’s assertion that more iron is needed, ‘Could it be that my iron recycling system isn’t working right, as opposed to my need for new iron?’”
Optimize Your Health by Donating Blood and Boosting Copper
The good news is that lowering your iron, which has many health benefits and can improve your life span, is easy to do. All you need to do is donate blood two to four times a year. As explained by Robbins:
“Blood loss is the only way to bring iron levels down in the human body. We’ve been trained to think we’re anemic and we’ve been trained to think we need to replace the iron, when in fact the missing piece of the puzzle is bioavailable copper — which is copper in the presence of retinol — so that the enzymes get properly loaded and can properly function.”
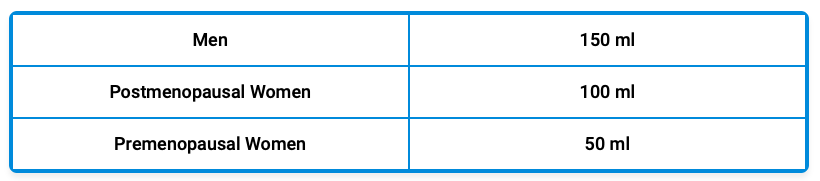
If losing 10% of your blood in one sitting is problematic for you, then you can remove blood in smaller amounts once a month on the schedule I have listed below. If you have congestive heart failure or severe COPD, you should discuss this with your doctor, but otherwise this is a fairly appropriate recommendation for most.
Lowering iron is one side of the equation. The other is increasing copper and retinol. For copper augmentation, Robbins recommends taking up to 3 to 4 mg of copper bisglycinate per day, or eating copper-rich foods, such as bee pollen, grass fed beef liver and acerola cherry. (Acerola cherry is very high in vitamin C, which contains copper-rich tyrosinase enzyme.)
Retinol is found in beef liver and beef organs, so if you eat that, you may not need any kind of supplement. Absent that, cod liver oil is a recognized source of real retinol.
More Information
In the interview, we also review a recent case study of a woman with persistent low ferritin, despite doing everything Robbins recommended, and what it took to resolve this case. So, for more details, be sure to listen to the whole interview.
We discuss the negative influence the stress hormone cortisol has on bioavailable copper (which can result in stubbornly low ferritin levels), and how addressing emotional knots using the Emotional Freedom Technique (EFT) can be instrumental in healing cases where stress and emotional turmoil play a part.
Robbins also reviews how dysfunctional iron metabolism and copper insufficiency affects conditions such as schizophrenia, obesity, ulcerative colitis and Crohn’s disease.
To learn more, be sure to visit Robbins’ website, RCP123.org, where you’ll find hundreds of YouTube videos and articles. There you can also access Robbins’ Root Cause Protocol, as well as his online RCP Institute training program, which is a 16-week course. Of course, you can also learn more from his book, “Cu-RE Your Fatigue: The Root Cause and How to Fix It on Your Own.”
*
Note to readers: Please click the share buttons above. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Notes
1 The Root Cause Protocol, Morley Robbins
Featured image is a screenshot from the video