


The most fundamental human right is the right to life. While legitimately criticized for the one party state, the death penalty, censorship, urban air pollution and harsh treatment of dissidents, China has been hugely successful in radically reducing infant mortality and maternal mortality in Tibet and in China as a whole.
In stark contrast, the war criminal US Alliance occupation of neighbouring Afghanistan continues to be associated with an under-1 infant mortality and maternal mortality incidence that is 7 times higher and 4-12 times higher, respectively, than that in Tibet – evidence of gross violation of the Geneva Convention and the UN Genocide Convention by the US Alliance.
Tibet became part of China in the 13th century under the Yuan dynasty [1], this happening at about the same time that the English were establishing control over the Celtic regions of Britain (Cornwall, Wales, Scotland and Ireland) and 6 centuries before the American Empire achieved its fullest “official” extent in the late 19th century with incorporation of elements of the Spanish Empire (Puerto Rico, the Philippines, and part of Cuba) [2].
Now human mortality (human death) is the bottom line in any consideration of the moral justification or humanitarian legitimacy of political systems, including empires. Key indicators are maternal mortality (the mortality rate of women during pregnancy, at or after delivery, and measured as maternal deaths per 100,000 live births), and infant mortality (measured as under-5 infant deaths per 1,000 live births).
A further key indicator is avoidable mortality (avoidable deaths, excess mortality, excess death, premature death, untimely death or deaths that should not have happened) that is measured as annual avoidable deaths from deprivation per 100 of population (avoidable deaths as a percentage of population per year). Avoidable deaths can be computed as the difference between the actual mortality in a country and the deaths expected for a peaceful, decently governed country with the same demographics (birth rate, age distribution). On a global comparative basis a “good”, baseline mortality rate for poor, high birth rate countries is about 4 deaths per 1,000 of population per year [2].
In 2003 the avoidable death rate (as a percentage of population per year) was about 0.97% (non-Arab Africa), 0.39% (Pacific), 0.38% (South Asia), 0.31% (Eastern Europe), 0.26% (Central Asia, Iran and Turkey), 0.26% (South East Asia), 0.25% (Arab North Africa and Middle East), 0.05% (Western Europe), 0.03% (Latin America and Caribbean), 0.01% (East Asia), 0.0% (Overseas Europe i.e. US, Australia, Canada, New Zealand and Apartheid Israel), and notably 0.0% for China, Cuba, Taiwan, South Korea and Japan [2]. In contrast, annual avoidable deaths from deprivation as a percentage of population in US Alliance-occupied Afghanistan was a shocking 1.75% and indicative of gross violation of the Geneva Convention and the UN Genocide Convention by the US Alliance. [2].
The UN Population Division provides detailed demographic data for all countries (e.g. population, births, deaths, and infant deaths but not avoidable deaths from deprivation) [3] and a useful finding for quickly estimating avoidable deaths from deprivation is that for impoverished, high birth rate countries, annual avoidable deaths are about 1.4 times the annual under-5 year old infant deaths [2].
With this background established we can now turn to infant mortality, maternal mortality and avoidable mortality in Southwest China’s Tibet Autonomous Region and compare this with that in China, US Alliance countries and in Tibet’s neighbour, US Alliance-occupied Afghanistan.
(1). China’s health success in the Tibet Autonomous Region versus a genocidal health disaster in US Alliance-occupied Afghanistan .
The China Daily reports (2017):
“Maternal mortality rate [in China ] declined to 199 per 1 million population [19.9 per 100,000 live births] last year, despite a rising number of births brought by the universal second-child policy, the country’s top health authority said on Friday. The figure for 2015 was 201 per 1 million [20.1 per 100,000 live births], according to the National Health and Family Planning Commission. Meanwhile, mortality rates for children under 5 decreased to 10.2 per thousand [live births] last year” [4].
These reports are consonant with CIA Factbook estimates of presently 12 under-1 infant deaths per 1,000 live births and 27 maternal deaths per 100,000 live births in China [5, 6]. By way of comparison, the CIA Factbook estimates a shocking circa 10-fold greater 110.6 under-1 infant deaths per 1,000 live births and 396 maternal deaths per 100,000 live births in US Alliance-occupied Afghanistan that borders upon the Tibet Autonomous region [5, 6].
According to China and UK health experts (2009):
“China represents one of the few success stories in maternal health. The maternal mortality ratio (MMR), estimated at 1500 deaths per 100 000 live births in the 1950s, decreased to an estimated 88 deaths per 100 000 live births in 1990”.
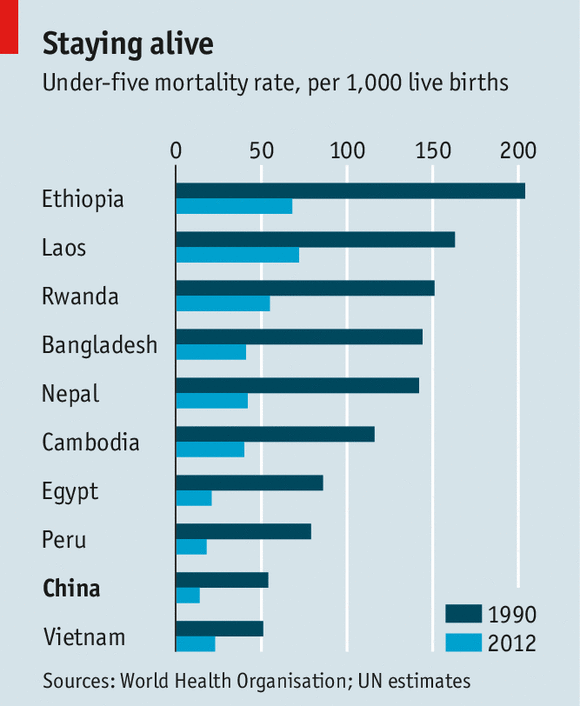
Source: The Economist
However the MMR was much higher in Tibet than in other regions of China (the Eastern being the best, the Central the next best, the Western region being worse and Tibet the worst) [7].
However the MMR has subsequently fallen further in Tibet according to the official Chinese news agency Xinhua (2016):
“Southwest China ‘s Tibet Autonomous Region saw record low maternity and infant death rates in 2015 thanks to improved healthcare conditions, according to the regional health and family planning commission. The mortality rate of Tibetan women during pregnancy, at or after delivery was halved from about 23 per 10,000 people [230 per 100,000 live births] in 2009 to 10 per 10,000 [100 per 100,000 live births] last year [2015], statistics released by the commission showed. In addition, the mortality rate of infants in Tibet was reduced to 16 per thousand [live births] in 2015 from 21 per thousand [live births] in 2009. During the period, the proportion of Tibetan women who gave birth in the hospital increased from about 51 percent to 90 percent. When the plateau region was liberated in 1951, its maternal and infant death rates stood at 5,000 per 100,000 people [live births] and 430 per thousand [live births] respectively” [8].
According to a joint report by the WHO (the World Health Organization), UNICEF (the United Nations Childrens’ Fund), UNFPA (The United Nations Population Fund, formerly the United Nations Fund for Population Activities), the World Bank Group and the UN Population Division, in the period 1990-2015 the MMR (Maternal Mortality Ratio, maternal deaths per 100,000 live births) fell from 97 to 27 in China as compared to a fall from 1,340 to 396 in Afghanistan [9].
However a recent report in the UK Guardian suggests an even greater Maternal Mortality and health disaster in Occupied Afghanistan:
“In one unpublished study, the Afghan government found an average level of maternal deaths between 800 and 1,200 for every 100,000 live births, according to aid workers in Kabul who have seen the research. If accurate, this would mean that women in Afghanistan – despite more than 15 years of international aid aimed at improving maternal mortality figures – may be dying from maternal complications at rates similar to those found in Somalia and Chad , and only surpassed by South Sudan . In another review, the UN Population Fund (UNFPA) found as many as 1,800 maternal deaths a year in the remote Afghan province of Ghor . Nine out of 11 provinces had higher death rates than the number normally used by donors. Both the UNFPA mortality numbers and the government’s own survey have yet to be released. A spokesman for the ministry of public health said the survey was not ready to be publicised yet, and declined to discuss findings…In addition, a 2013 study by the Institute for Health Metrics and Evaluation at the University of Washington reported 885 annual maternal deaths in Afghanistan. According to the researchers, that was an increase of 24% on a decade earlier. In Afghanistan , reality often conflicts with official statistics. The UK government, for instance, claims that 85% of Afghans are now covered by basic health services. Yet, in a 2014 Médecins Sans Frontières report, four out of five Afghans said they did not use their closest public clinic because they believed the quality of services and availability of staff was so poor. According to the UN Office for the Coordination of Humanitarian Affairs, 9 million Afghans [population 35 million] are without access to basic health services” [10].
In summary, infant mortality (under-1 infant deaths per 1,000 live births) is 12 ( China ), 16 ( Tibet ), 6 ( USA ) and 111 (US Alliance-occupied Afghanistan ). The Maternal Mortality Ratio (MMR) (maternal deaths per 100,000 live births) is 20- 27 ( China ), 100 ( Tibet ), 14 ( USA ) and 400-1,200 (US Alliance-occupied Afghanistan ).
As explained below, this constitutes evidence of horrendous US Alliance war crimes in Occupied Afghanistan in gross violation of the Geneva Convention relative to the Protection of Civilian Persons in Time of War [11] and thence of the UN Genocide Convention [12].
(2). Mass infant mortality and mass maternal mortality in US Alliance Occupied Afghanistan is a war crime violating the Geneva and Genocide Conventions.
Killing in war occurs not just through violence (active killing) but also through avoidable death from imposed deprivation (passive mass murder) [2]. Mass mortality in a Subject population occurs in gross violation of Articles 55 and 56 of the Geneva Convention relative to the Protection of Civilian Persons in Time of War that unequivocally states that the Occupier must supply its Subjects with life-sustaining food and medical services “to the fullest extent of the means available to it” [11].
Genocide is defined by Article 2 of the UN Genocide Convention that states:
“In the present Convention, genocide means any of the following acts committed with intent to destroy, in whole or in part, a national, ethnic, racial or religious group, as such: a) Killing members of the group; b) Causing serious bodily or mental harm to members of the group; c) Deliberately inflicting on the group conditions of life calculated to bring about its physical destruction in whole or in part; d) Imposing measures intended to prevent births within the group; e) Forcibly transferring children of the group to another group” [11].
The UN Population Division informs that the annual number of births in Occupied Afghanistan is 1,155,458 (2015). The infant mortality (under-1 infant deaths per 1,000 live births) of 111 for US Alliance-occupied Afghanistan means that 111 x 1,155.5 = 128,261 under-1 year old infants die each year in Occupied Afghanistan. If the US provided life-sustaining food and medical services to its conquered Afghan subjects “to the fullest extent of the means available to it” (i.e. to yield an under-1 infant mortality of 6 deaths per 1,000 live births as in the US ) then Occupied Afghanistan under-1 infant deaths would only total 6 x 1,155.5 = 6,933. Failure of the US Alliance to observe the unequivocal demands of the Geneva Convention results in the avoidable death of under-1 Afghan infants totalling 128,261 – 6,933 = 121,328 each year or 40 times the carnage in the US Government’s 9-11 false flag atrocity (3,000 killed). Over the 16 years of the Afghan War this US Alliance mass murder of infants amounts to the death of 16 years x 121,328 per year = 1.9 million under-1 year old Afghan infants.
Similarly, the Maternal Mortality Ratio (MMR) (maternal deaths per 100,000 live births) of 400-1,200 for US Alliance-occupied Afghanistan means that (400-1,200) x 11.55 = 4,620- 13,860 Afghan women suffer maternal mortality each year as compared to 14 x 11.55 = 162 if the US Alliance observed the Geneva Convention. Thus the failure of the US Alliance to observed the Geneva Convention kills 4,458- 13,698 Afghan women each year. The Afghan maternal mortality due to US Alliance war crimes over the 16 years of the Afghan War is accordingly 71,000-219,000.
Now the racist moral degenerates who dominate the West ( US imperialists, US lackeys, genocidal racist Zionists) may well argue that Afghanistan is a poor and remote country and that the noble, US-led Coalition that has “liberated” Afghanistan cannot be expected to work medical miracles overnight. However China with an annual per capita GDP of merely $8,126 (as compared to America ’s $56,054) [13] has indeed obtained remarkable health outcomes in remote, rural and poor Tibet that borders on Occupied Afghanistan. The infant mortality rate in the Tibet Autonomous Region is 7 times lower than in Occupied Afghanistan and the Maternal Mortality Ratio in Tibet is 4-12 times lower than that in US-occupied Afghanistan . We can now consider the relative wealth and health outcomes of the individual member countries of the US Alliance that has been devastating Occupied Afghanistan in gross violation of the Geneva Convention and the UN Genocide Convention .
(3). The war criminal European US Alliance invaders have very high per capita income, very low infant mortality and very low maternal mortality.
In order to quantitatively compare the abilities of the US Alliance members to meet their Subject life-sustaining obligations as Occupiers under the Geneva Convention, one can compare the very high annual per capita incomes of the US Alliance nations with the correspondingly very low infant mortality and maternal mortality achieved in these countries.
Below are listed US Alliance participants in the Afghan Holocaust and Afghan Genocide in order of (a) numbers of military deaths in Occupied Afghanistan (2015) as a measure of degree of participation [14], with (b) under-1 infant deaths per 1,000 live births [5, 15], (c) perinatal maternal deaths expressed as deaths per 100,000 live births [6], and (d) GDP nominal per capita in US dollars per person [13]:
United States (a) 2,271 military deaths, (b) 5.8 under-1 infant deaths per 1,000 live births , (c) 14 maternal deaths per 100,000 live births, (d) $56,054 per person GDP nominal per capita;
United Kingdom (a) 453, (b) 4.3, (c) 9, (d) $44,162; Canada (a) 178, (b) 4.5, (c) 7, (d) $43,206 ; France (a) 88, (b) 3.2, (c) 8, (d) $36,304; Germany (a) 57, (b) 3.4, (c) 6, (d) $41,686; Italy (a) 53, (b) 3.3, (c) 4, (d) $30,462;
Poland (a) 44, (b) 4.4, (c) 3, (d) $12,355; Denmark (a) 43, (b) 4.0, (c) 6, (d) $53,149; Australia (a) 41, (b) 4.3, (c) 6, (d) $51,352; Spain (a) 35, (b) 3.3, (c) 5, (d) $25,865 ; Georgia (a) 32, (b) 15.2, (c) 36, (d) $3,491;
Netherlands (a) 25, (b) 3.6, (c) 7, (d) $44,332; Romania (a) 28, (b) 9.4, (c) 31, (d) $9,121; Turkey (a) 15, (b) 17.6, (c) 16, (d) $9,126; Czech Republic (a) 10, (b) 7.9, (c) 4, (d) $17,562; New Zealand (a) 10, (b) 4.4, (c) 11, (d) $38,294;
Norway (a) 10, (b) 2.5, (c) 5, (d) $74,186; Estonia (a) 9, (b) 3.8, (c) 9, (d) $17,122; Hungary (a) 7, (b) 4.9, (c) 17, (d) $12,351; Sweden (a) 5, (b) 2.6, (c) 4, (d) $50,687; Latvia (a) 4, (b) 5.2, (c) 18, (d) $13,704; Slovakia (a) 3, (b) 5.1, (c) 6, (d) $16,082;
Finland (a) 2, (b) 2.5, (c) 3, (d) $42,148; Jordan (a) 2, (b) 14.2, (c) 58, (d) $4,940; Portugal (a) 2, (b) 4.3, (c) 10, (d) $19,239; South Korea (a) 2, (b) 3.0, (c) 11, (d) $27,397; Albania (a) 1, (b) 11.9, (c) 29, (d) $3,984;
Belgium (a) 1, (b) 3.4, (c) 7, (d) $40,278; Lithuania (a) 1, (b) 3.8, (c) 10, (d) $14,384; Montenegro (a) 1, (b) 5.8 [Serbia figure], (c) 7, (d) $6,424; Croatia (a) 0, (b) 9.3, (c) 8, (d) $11,479; Greece (a) 0, (b) 4.6, (c) 3, (d) $17,788;
Iceland (a) 0, (b) 2.1, (c) 3, (d) $50,936; Japan (a) 0, (b) 2.0, (c) 5, (d) $34,629; Macedonia (a) 0, (b) 7.4, (c) 8, (d) $4,836; Slovenia (a) 0, (b) 3.9, (c) 9, (d) $20,690.
These data for the Occupiers are in stark contrast to the corresponding horrendous data for Occupied Afghanistan: (a) 5.6 million deaths from violence, 1.4 million (as determined from comparisons with the Iraq War for which expert survey data is available [16, 17]), or from imposed deprivation, 4.2 million [2, 16-18]), (b) 110.6 under-1 infant deaths per 1,000 live births , (c) 400-1,200 maternal deaths per 100,000 live births, (d) $623 per person GDP nominal per capita [13].
Indeed, as noted above in section (2), China with an annual per capita GDP of merely $8,126 (as compared to America’s $56,054) [13] has obtained an infant mortality in the Tibet Autonomous Region that is 7 times lower than that in Occupied Afghanistan and a Maternal Mortality in Tibet that is 4-12 times lower than that in US-occupied Afghanistan.
The Occupiers are overwhelmingly extremely prosperous European states which can evidently each afford to provide Occupied Afghanistan with greatly increased life-sustaining food and medical services if provided “to the fullest extent of the means available” and which would guarantee correspondingly very low infant mortality and maternal deaths – but clearly fail to do so as evidenced by the shocking infant mortality and maternal mortality in Occupied Afghanistan. . Even the poorest of the Occupiers (Georgia, Jordan, Albania and Macedonia ) have per capita incomes an order of magnitude greater than that of Occupied Afghanistan and infant mortality and maternal mortality that are an order of magnitude lower than that in Occupied Afghanistan.
The US Alliance Occupiers are in gross violation of Articles 55 and 56 of the Geneva Convention relative to the Protection of Civilian Persons in Time of War that both demand that an Occupier must proved the conquered Subjects with life-sustaining food and medical services “to the fullest extent of the means available to it” [11].
An analogy from civil society is germane – a kidnapper will be prosecuted for depriving his victims of their liberty but if any of his victims die from deprivation in his custody he will also be charged with murder. Indeed highly abusive parents will be charged with murder if deliberate deprivation of their children results in death.
Wartime analogies from WW2 are also germane. Thus the WW2 Jewish Holocaust was associated with 5-6 million deaths from (a) violence or (b) imposed deprivation but the precise relative extents of (a) active killing (by shooting, gassing and other violent means) versus (b) passive killing (through deprivation of life-sustaining food and medical services) is not clear [19-22]. However whether a person is killed by violence or through imposed deprivation, the death is just as final and the crime just as abhorrent. Western Mainstream treatment of the WW2 Jewish Holocaust focuses on violent deaths and largely ignores the WW2 European Holocaust of which it was a part (30 million Slavs, Jews and Gypsies killed by violence or deprivation) [2]. Of course, ignoring past or present genocide or holocaust atrocities is far, far worse than repugnant genocidal denial or holocaust denial because the latter at least admits the possibilities of refutation and public discussion.
Also largely ignored by racist Western Mainstream journalists, politicians and academics is the WW2 Chinese Holocaust and Chinese Genocide (35 million Chinese deaths from violence or imposed deprivation, 1937-1945) [23] and the WW2 Indian Holocaust and Indian Genocide (Bengali Holocaust, Bengali Genocide, 1942-1945 Bengal Famine) in which the British with Australian complicity deliberately starved 6-7 million Indians to death for strategic reasons (Australia withholding food from starving Indian from its huge wartime grain stores) [2, 24-30]. Indeed the Bengali Holocaust (Bengal Famine) was the first WW2 atrocity to be described as a “holocaust (by N.G. Jog in a 1944 book entitled “Churchill’s Blind-Spot: India ” [30]) . However these massive WW2 holocausts are largely ignored and the term “the Holocaust” is taken in the Zionist-subverted, Zionist-perverted and racist West to exclusively mean only the WW2 Jewish Holocaust atrocity.
Present day genocides that are also resolutely ignored by Western Mainstream media include (deaths from violence plus war-imposed deprivation in brackets) the Palestinian Genocide (2 million, WW1-present) [31], the Iraqi Genocide (4.6 million, 1990-2011; 9 million, WW1-2011) [17, 18], Somali Genocide (2.2 million, 1992-present) [2, 18], and the Afghan Genocide (5.6 million, 2001-present) [2, 16, 18]. The ongoing Muslim Holocaust and Muslim Genocide (aka the US War on Terra or the US War on Muslims) has so far involved 32 million Muslim deaths from violence, 5 million, or deprivation, 27 million, since the US Government’s 9-11 false flag atrocity that may also have involved Apartheid Israel and Saudi Arabia [32, 33].
Although the Awful Truth about horrendous infant mortality and maternal mortality in Occupied Afghanistan and other targets of US imperialism is readily available from Mainstream sources such as the UN Population Division [3] and the CIA Factbook [5, 6] , Western Mainstream journalist, politician, commentariat and academic presstitutes resolutely look the other way. Even anti-war activists fail to report the horrendous numbers, either because they prefer rhetoric to arithmetic or because they don’t want to frighten the horses. Many activists are insufficiently activist or activism lite by being climate lite, socialism lite, anti-Apartheid lite, and anti-war lite. The sad reality is that activists who have public visibility in the Mainstream media would be quickly rendered invisible if their messaging was too strong. At the heart of this problem of soft, weak, deficient and compromised activist messaging is immense and increasing wealth inequality that subverts democracy and cripples effective free speech [34-36]. Of course, no messaging is too strong when it comes to mass murder of women and children such as that being perpetrated by the war criminal US Alliance in Occupied Afghanistan.
Final comments
Some journalists have spoken out about this ongoing passive mass murder of the innocent. Thus on May 12, 1996, Madeleine Albright (US UN Ambassador and later US Secretary of State, 1997-2001) defended UN sanctions against Iraq on a “60 Minutes” segment in which anti-racist Jewish American journalist Lesley Stahl asked her
“We have heard that half a million children have died. I mean, that’s more children than died in Hiroshima. And, you know, is the price worth it?”
Madeleine Albright notoriously replied
“We think the price is worth it” [37].
In 2005, an anti-racist Jewish Australian writer (myself) made a nation-wide broadcast on Australia’s ABC (the Australian equivalent the UK BBC) in which I exposed Australian complicity in Iraqi mass mortality due to war-imposed deprivation [38, 39]. I have endlessly argued the case for the millions of such innocent victims of passive mass murder by the serial war criminal US Alliance [40]. The Silence has been Deafening but we cannot give up. Peace is the only way but silence kills and silence is complicity.
The present article identifies the overwhelmingly rich, European countries involved in the ongoing passive mass murder of Afghan women and children by the serial war criminal US Alliance. The war casualties of these nations provides a measure of complicity in the ongoing Afghan Holocaust and Afghan Genocide. Mass murder of children and women is utterly abhorred by all civilized people, who will be compelled to act by
(a) informing everyone they can, and
(b) urging Boycotts Divestment and Sanctions (BDS) against all those countries, corporations, parties and politicians involved in this continuing horrendous crime against Humanity.
*
Notes
[1]. “Tiber”, Wikipedia: https://en.wikipedia.org/wiki/Tibet
[2]. Gideon Polya, “Body Count. Global avoidable mortality since 1950”, including an avoidable mortality-related history of every country from Neolithic times and is now available for free perusal on the web :http://globalbodycount.blogspot.com.au/
[3]. UN Population Division, “World Population Prospects 2017”: https://esa.un.org/unpd/wpp/
[4]. Wang Xiaodong, “Maternal mortality declines and births increase”, China Daily, 20 January 2017: http://www.chinadaily.com.cn/china/2017-01/20/content_28011989.htm
[5]. CIA, The World Factbook, “Infant mortality”, https://www.cia.gov/library/publications/the-world-factbook/fields/2091.html
[6]. CIA, The World Factbook, “Maternal mortality”: https://www.cia.gov/library/publications/the-world-factbook/rankorder/2223rank.html
[7]. Gao Yanqiu, Carine Ronsmans and An Lin, “Time trends and regional differences in maternal mortality in China from 2000 to 2005”, Bulletin of the World Health Organization 2009;87:913-920: http://www.who.int/bulletin/volumes/87/12/08-060426/en/
[8]. Xinhua, “ Tibet slashes maternity, infant mortality rates”, New China, 18 January 2016: http://news.xinhuanet.com/english/2016-01/18/c_135020798.htm
[9]. WHO, UNICEF, UNFPA, World Bank Group and the UN Population Division, “Trends in Maternal Mortality, 1990-2015”: http://apps.who.int/iris/bitstream/10665/194254/1/9789241565141_eng.pdf?ua=1
[10]. Sune Engel Rasmussen, “Maternal death rates in Afghanistan may be worse than previously thought”, Guardian, 31 January 2017: https://www.theguardian.com/global-development/2017/jan/30/maternal-death-rates-in-afghanistan-may-be-worse-than-previously-thought
[11]. “Geneva Convention (IV) relative to the Protection of Civilian Persons in Time of War: https://www.un.org/ruleoflaw/files/Geneva%20Convention%20IV.pdf
[12]. “Article 2 of the UN Genocide Convention”: http://www.edwebproject.org/sideshow/genocide/convention.html
[13]. “List of countries by GDP (nominal) per capita”, Wikipedia: https://en.wikipedia.org/wiki/List_of_countries_by_GDP_(nominal)_per_capita
[14]. “Coalition casualties in Afghanistan ”, Wikipedia: https://en.wikipedia.org/wiki/Coalition_casualties_in_Afghanistan
[15]. “List of countries by infant mortality rate”, Wikipedia: https://en.wikipedia.org/wiki/List_of_countries_by_infant_mortality_rate
[16]. “Afghan Holocaust, Afghan Genocide”: http://sites.google.com/site/afghanholocaustafghangenocide/
[17]. “Iraqi Holocaust, Iraqi Genocide”: http://sites.google.com/site/iraqiholocaustiraqigenocide/
[18]. “Muslim Holocaust Muslim Genocide”: https://sites.google.com/site/muslimholocaustmuslimgenocide/
[19]. Martin Gilbert, “Jewish History Atlas” (Weidenfeld and Nicolson, London, 1969)
[20]. Martin Gilbert “Atlas of the Holocaust”(Michael Joseph, London, 1982)
[21]. Gideon Polya, “UK Zionist Historian Sir Martin Gilbert (1936-2015) Variously Ignored Or Minimized WW2 Bengali Holocaust ”, Countercurrents, 19 February, 2015: http://www.countercurrents.org/polya190215.htm
[22]. Eric Silver, “An interview with David Irving, Confronting Hitler’s defender”, Action Report, 4 June 2000: http://www.fpp.co.uk/online/00/05/Silver.html
[23]. “Backgrounder: China ’s WWII contributions in figures”, New China, 3 September 2015: http://news.xinhuanet.com/english/2015-09/03/c_134582291.htm
[24]. Gideon Polya, “Australia And Britain Killed 6-7 Million Indians In WW2 Bengal Famine”, Countercurrents, 29 September, 2011: http://www.countercurrents.org/polya290911.htm
[25]. Gideon Polya, “Jane Austen and the Black Hole of British History. Colonial rapacity, holocaust denial and the crisis in biological sustainability”, now available for free perusal on the web: http://janeaustenand.blogspot.com/2008/09/jane-austen-and-black-hole-of-british.html
[26]. Madhusree Muckerjee, “Churchill’s Secret War. The British Empire and the ravaging of India during World War II” (Basic Books, New York , 2010)
[27]. Colin Mason, “A Short History of Asia . Stone Age to 2000AD” (Macmillan, 2000)
[28]. “Bengali Holocaust (WW2 Bengal Famine) writings of Gideon Polya”, Gideon Polya: https://sites.google.com/site/drgideonpolya/bengali-holocaust
[29]. Gideon Polya (2013), “Review: “The Cambridge History Of Australia” Ignores Australian Involvement In 30 Genocides”, Countercurrents, 14 October, 2013: http://www.countercurrents.org/polya141013.htm
[30]. N.G. Jog, “Churchill’s Blind-Spot: India ”, New Book Company, Bombay , 1944
[31]. “Palestinian Genocide”: http://sites.google.com/site/palestiniangenocide/
[32]. Gideon Polya, “Paris Atrocity Context: 27 Million Muslim Avoidable Deaths From Imposed Deprivation In 20 Countries Violated By US Alliance Since 9-11 ”, Countercurrents, 22 November, 2015: http://www.countercurrents.org/polya221115A.htm
[33]. “Experts: US did 9-11”: https://sites.google.com/site/expertsusdid911/
[34]. Gideon Polya, “Planetary salvation compromised by activism-lite, climate-lite, anti-Apartheid-lite & anti-war-lite nweakness”, Countercurrents, 15 November 2017: http://www.countercurrents.org/2017/11/15/planetary-salvation-compromised-by-activism-lite-climate-lite-anti-apartheid-lite-anti-war-lite-weakness/
[35]. “Mainstream media censorship”: https://sites.google.com/site/mainstreammediacensorship/home
[36]. “Mainstream media lying”: https://sites.google.com/site/mainstreammedialying/
[37]. Lesley Stahl and Madeleine Albright quoted in “Madeleine Albright”, Wikipedia:http://en.wikipedia.org/wiki/Madeleine_Albright
[38]. Gideon Polya, “Australian complicity in Iraqi mass mortality”, ABC Radio National, Ockham’s Razor, 28 August 2005: http://www.abc.net.au/radionational/programs/ockhamsrazor/australian-complicity-in-iraq-mass-mortality/3369002#transcript
[39]. Gideon Polya, “Australian complicity in Iraqi mass mortality” in “Lies, Deep Fries & Statistics” (edited by Robyn Williams, ABC Books, Sydney, 2007
[40]. Gideon Polya: https://sites.google.com/site/drgideonpolya/home